Human papillomavirus (HPV) is a small, non-enveloped, double-stranded DNA virus that has oncogenic potential.[1] Most HPV infections, whether caused by low-risk or high-risk types, are transient, asymptomatic, and have no clinical consequences.[2] In a substantial number of individuals, however, sexually transmitted HPV infection may cause anogenital warts, anogenital cancers, and oropharyngeal cancers.[3] The majority of urogenital and oropharyngeal cancers in the United States are caused by HPV (Figure 1).[4] Indeed, in the United States, approximately 50,000 HPV-related cancers are diagnosed each year, including cancer of the cervix, cancer of the anus, and cancer of the oropharynx.[5,6,7] The 9-valent HPV vaccine is highly effective in preventing anogenital warts, precancerous lesions, and invasive cancers associated with HPV. Screening for HPV-related cervical cancer is an important component of cancer prevention for adult women. The following discussion on HPV will focus primarily on the diagnosis and management of anogenital warts, use of the HPV vaccine to prevent urogenital cancers, and screening for HPV-related cancers.
- Module 2 Overview
Self-Study Lessons - Lesson 1
Chlamydial InfectionsActivities- Lesson 2
Gonococcal InfectionsActivities- Lesson 3
SyphilisActivities- Lesson 5
Genital HerpesActivities- Lesson 6
Human Papillomavirus InfectionActivities- Lesson 7
Pelvic Inflammatory DiseaseActivities- Lesson 8
VaginitisActivities- Lesson 9
MpoxActivities- Lesson 10
Mycoplasma genitaliumActivitiesLesson 6. Human Papillomavirus Infection
PDF ShareLast Updated: March 20th, 2025Authors:Helen C. Stankiewicz Karita, MD,Helen C. Stankiewicz Karita, MD
Associate Professor of Medicine
University of California at San FranciscoDisclosures: NoneJehan Z. Budak, MD,Jehan Z. Budak, MD
Assistant Professor of Medicine
Division of Allergy & Infectious Diseases
University of WashingtonDisclosures: NoneDavid H. Spach, MDDavid H. Spach, MD
Editor-in-Chief
Professor of Medicine
Division of Allergy and Infectious Diseases
University of WashingtonDisclosures: NoneLearning Objective Performance Indicators
- Recognize clinical manifestations of HPV-related anogenital warts and anogenital cancers
- Provide routine HPV-related cancer screening for populations at risk
- Appropriately select patient-applied or provider-administered treatments for anogenital warts
- Administer the 9-valent HPV vaccine to prevent HPV-related genital warts and cancer
- Counsel and educate individuals with genital warts
Table of ContentsIntroduction
Epidemiology in the United States
HPV Incidence
It is estimated that most sexually active men and women will acquire genital HPV infection at some point in their lives, but approximately 90% of these infections are clinically silent, and most infections resolve spontaneously.[1] Because HPV infection is not reportable in the United States, precise yearly statistics on the incidence (new HPV infections) are not available. Nevertheless, using the HPV Agent-based Dynamic model for Vaccination and Screening Evaluation (HPV-ADVISE), the Centers for Disease Control and Prevention (CDC) estimated that approximately 13 million new HPV infections in the United States occurred in 2018, including 6.9 million new HPV infections in men and 6.1 million in women (Figure 2).[8]
HPV Prevalence
The prevalence of HPV infection in the United States is very high. Based on data from the National Health and Nutrition Examination Survey (NHANES), there were an estimated 77.3 million persons 15 to 59 years of age in the United States with a prevalent HPV infection in 2018, including 42.5 million with a disease-associated HPV infection.[8] Overall, the prevalence of any HPV type was approximately 40%, with a higher prevalence in men than in women (Figure 3).[8] In a review of 53 studies that addressed anal HPV prevalence in men who have sex with men (MSM), investigators found a pooled anal HPV prevalence for any HPV type of 63.9% for MSM without HIV and 92.6% for MSM with HIV.[9] A meta-analysis of 95 studies found that anal HPV prevalence among women with normal anal cytology was 42% for women without HIV and 59% for women with HIV.[10] The prevalence of oral HPV is lower than with anogenital HPV.[11,12] In a cross-sectional analysis of dental offices in the United States in 2021-2022, the prevalence of any oral HPV type was 6.6% and HPV-16 was 0.7%; the prevalence of oral HPV was highest among men 51 to 60 years of age.[13]
Impact of HPV-Related Diseases
The following summarizes major diseases related to sexually transmitted HPV. The incidence and prevalence of anogenital warts are difficult to estimate in the United States since diagnoses of anogenital warts are not reportable. Data for cervical and anal cancer come from the National Cancer Institute (NCI) Surveillance, Epidemiology, and End Results (SEER) Program.[14]
- Anogenital Warts: Most available prevalence data are based on selected analyses from urban sexually transmitted diseases clinics. For example, a 2010–2011 sexually transmitted diseases (STD) clinic-based study reported the prevalence of anogenital warts in 2010-2011 was 7.5% among men who have sex with women only, 7.5% among MSM, and 2.4% among women.[15]
- Cervical Cancer: Approximately 90% of cervical cancers in the United States are caused by HPV.[4] In the United States, for the year 2024, the NCI SEER Program estimated 13,820 new cases of cervical cancer and 4,360 deaths from cervical cancer.[6] In 2024, the rate of new cases of cervical cancer was 7.6 per 100,000 persons.[6] During the years 2017-2021, the median age of cervical cancer diagnosis in the United States was 50 years.[6]
- Anal Cancers: Approximately 90% of anal cancers in the United States are caused by HPV.[4] In the United States, for the year 2024, the NCI SEER Program estimated 10,540 new cases of anal cancer and 2,190 deaths from anal cancer.[5] In 2024, the rate of new cases of anal cancer was 1.9 per 100,000 persons.[5] During the years 2017-2021, the median age of anal cancer diagnosis in the United States was 64 years.[5]
- Oral Cavity and Pharyngeal Cancer: Approximately 70% of oropharyngeal cancers in the United States are caused by HPV.[4,16] In the United States, for the year 2024, the NCI SEER Program estimated 58,450 cases of oral cavity cancer and pharyngeal cancer and 12,230 deaths from oropharyngeal cancer.[7] In 2024, the rate of new cases of oral cavity cancer and pharyngeal cancer was 11.5 per 100,000 persons.[7] During the years 2017-2021, the median age of oropharyngeal cancer diagnosis in the United States was 64 years.[7]
Factors Associated with HPV Infection
Key factors associated with the acquisition of genital HPV infection include a higher number of lifetime sex partners and a younger age of sexual debut.[17] Although a greater number of lifetime sex partners is associated with a higher likelihood of acquiring HPV, even a person with a few or even one lifetime sex partner can develop HPV infection.[3] Investigators have evaluated potential risk factors associated with cervical cancer, including immunosuppression, long-term oral contraceptive use, multiple pregnancies, tobacco smoking, and coinfection with HIV, herpes simplex virus 2, or Chlamydia trachomatis infection.[18,19] For HPV-related oropharyngeal cancers, the risk is specifically related to oral sex.[20]
Microbiology, Pathogenesis, and Transmission
Viral Structure
Human papillomavirus is a small, nonenveloped, double-stranded DNA virus that is approximately 50 to 60 nm in diameter.[21,22] The viral DNA genome encodes eight open-reading frames comprised of six early (E1, E2, E4, E5, E6, E7) proteins that maintain regulatory function (and can cause cell oncotransformation) and two late (L1 and L2) proteins that are involved in viral assembly.[21,22] Human papillomavirus has a characteristic icosahedral viral outer shell, primarily comprised of 72 star-shaped pentameric capsomeres; each pentameric capsomer contains 5 HPV L1 proteins, and each virion contains 360 of the L1 proteins (Figure 4).[2,21,23] The 72 pentameric capsomers have the unique ability to self-assemble and form the outer HPV shell; this self-assembling property is the key element used in the design and production of the HPV vaccine.[24] The viral shell also contains up to 72 molecules of the L2 minor protein, which are believed to play a role in linking the capsid to the HPV DNA.[2,25]
Classification of HPV Types
The identification and typing of HPV in tissues occurs via the detection of HPV DNA or HPV mRNA. More than 200 types of HPV have been classified, and more than 40 types of HPV can infect the anogenital and oral tracts of humans.[21,26,27] The HPV types, which have a specific affinity for genital, anal, and oropharyngeal skin and mucosa, are divided into two groups based on whether they have an association with cancer: low-risk (nononcogenic types) and high-risk (oncogenic types).[2,4,28,29]
Table 1. Human Papillomavirus Types
Low-Risk Types (nononcogenic)
- Associated with genital warts and benign or low-grade cellular changes (mild Pap test abnormalities).
- Approximately 90% of genital warts are caused by HPV types 6 and 11.
- The HPV types causing genital warts can occasionally cause lesions on oral, upper respiratory, upper gastrointestinal, and ocular locations. Recurrent respiratory papillomatosis, a rare condition, is usually associated with HPV types 6 and 11.
High-Risk Types (oncogenic)
- Associated with low-grade cervical cellular changes, high-grade cervical cellular changes (mild, moderate, and severe Pap test abnormalities), cervical dysplasia, and cervical cancer. In addition, associated with cancers of the oropharynx, anus, vulva, vagina, and penis.
- HPV types 16 and 18 account for approximately 65-70% of cervical cancers.
- The HPV types 31, 33, 45, 52, and 58 cause approximately 10% of all HPV-associated cancers.
Pathogenesis
The HPV types that infect humans have a known specificity for mucosal and cutaneous epithelium.[21,30] Infection with HPV occurs at the basal cell layer of stratified squamous epithelial cells.[30] Infection stimulates cellular proliferation in the epithelium, and the infected cells display a broad spectrum of changes, with a spectrum of cellular outcomes that include inapparent infection, benign hyperplasia (papilloma), precancerous lesions, and invasive carcinoma.[30] To effectively replicate, HPV must utilize the host cellular machinery. During the process, the viral protein product encoded by E6 binds to the p53 tumor suppressor gene product, which results in the premature degradation of the p53 protein.[31] The E7 protein binds to a tumor suppressor protein—the retinoblastoma protein—and inhibits its function.[32] The E6 and E7 proteins mediate much of the HPV oncogenic potential by assisting the cell in evading host immunity, a process that facilitates virion production in differentiating epithelial cells.[2,30]
Transmission of Genital HPV
Transmission of genital HPV is predominantly associated with sexual activity that results in friction-induced microabrasions during skin-to-skin contact.[2,33] The transmission rate of HPV between sex partners is high, and transmission often occurs from persons with HPV who are asymptomatic or have subclinical infection.[34,35] Consistent and correct use of condoms reduces the risk of genital HPV acquisition or transmission, thereby reducing the risk for HPV-associated diseases.[3,36] Condom use, however, does not entirely prevent transmission of HPV, since exposure to HPV can occur in areas that are not fully covered or protected by a condom.[3] Treatment of warts or cervical cellular abnormalities will reduce, but not eliminate, the risk of transmission. Transmission of HPV through nonsexual routes can occur, but is uncommon.[37,38] Mothers with low-risk genital HPV types can rarely transmit HPV to their newborn during delivery, but if transmission does occur, HPV has the potential to cause recurrent respiratory papillomatosis in children.[39,40] Nonsexual activities can also lead to anal HPV infection, particularly through the transmission of HPV from the cervicovaginal tract.[41] Wiping from front to back after using the toilet may be linked to higher rates of anal HPV infection, compared to wiping or patting in the opposite direction.[42]
Natural History of HPV Infections
Available data, primarily from cervical HPV natural history, suggest that more than 90% of individuals with genital HPV infections are asymptomatic and clear the infection within 3 years.[2,43,44] The “viral clearance” can entail complete elimination of HPV from the tissues or cell-mediated immune suppression of the HPV to such a low level that HPV DNA levels are undetectable using sensitive HPV DNA tests (referred to as “viral latency”).[2,45]
- Natural History with Anogenital Warts: Nearly all anogenital warts are caused by HPV type 6 or 11, and longitudinal studies show warts develop in 14.6 to 64.2% of persons following acquisition of either of these HPV genotypes.[46,47,48] For individuals who go on to develop anogenital warts, the median incubation period, representing the time from acquisition to clinical manifestations, is approximately 2.9 to 6.0 months in women and 11.0 months in men.[29,47,48]
- Natural History with Cervical HPV Infection: Following acquisition of HPV, the median duration of HPV infection of the cervix (measured by detection of HPV DNA) is approximately 1 to 2 years, depending on the HPV type.[49] For women who develop cervical cancer, the time from infection until precancerous cytologic abnormalities develop is typically several years, and if progression to cervical cancer occurs, it typically does not occur until decades after the initial infection.[2,50,51] The potential progression to cervical cancer is a dynamic process with a spectrum of potential outcomes that include immune-mediated clearance of HPV from the cervix, progression to a precancerous lesion, regression of precancerous lesions, and progression of precancerous lesions to cervical cancer with invasion of local tissue planes (Figure 5).[50,51,52,53]
- Natural History with Anal HPV Infection: Following acquisition of HPV, the median duration of HPV infection of the anus is highly HPV type-dependent. In one study involving young women with anal HPV, by 3 years, clearance of anal HPV had occurred with 82.5% of non-16 high-risk HPV, 82.6% of low-risk HPV, 76.2% of HPV-16, and 36.4% for all HPV types.[54] In two separate studies involving MSM with HPV infection, there were median durations of HPV-16 infection of 17 and 22 months, respectively.[55,56] Precancers of the anus may also spontaneously regress, with one study finding a regression rate of 22 per 100 person-years.[57]
- Natural History with Oral HPV Infection: The natural history of oral HPV infection is not well understood. In one study of immunocompetent men, oncogenic-type oral HPV infection cleared within 12 months.[58] Precursor lesions for HPV-associated oropharyngeal cancer have not been identified.
Clinical Manifestations
Overview of HPV-Related Manifestations
Most HPV infections are transient, asymptomatic, or subclinical; among immunocompetent individuals, most HPV infections have no clinical consequences. Persons with clinically evident disease have a range of possible presentations that correlate with the HPV type and host factors, with the most common manifestations being anogenital warts, also referred to as low-grade squamous intraepithelial lesions (LSIL), precancerous lesions, known as high-grade squamous intraepithelial lesions (HSIL), and invasive cancer.[59,60] Although most precancerous lesions are not visible clinically, some will subsequently progress to form visible lesions or masses in the anogenital region.
Anogenital Warts
Types of Anogenital Warts
Individuals with visible anogenital warts frequently have simultaneous infection with multiple HPV types. There are four major morphologic types of anogenital warts commonly described:
- Condylomata acuminata (cauliflower-like appearance and may be skin-colored, pink, or hyperpigmented)
- Smooth papules (usually dome-shaped and skin-colored)
- Flat papules (macular to slightly raised, skin-colored, and have a smooth surface)
- Keratotic warts (with a thick keratinized layer that can resemble common warts or seborrheic keratosis)
Anogenital warts can be confused with other conditions, including other genital infections, acquired dermatologic conditions, and normal anatomic variants.
Table 2. Differential Diagnoses for Anogenital Warts
Manifestations of Other Genital Infections
- Condylomata lata (manifestation of secondary syphilis)
- Molluscum contagiosum
- Herpes vegetans
Acquired Dermatologic Conditions
- Seborrheic keratosis
- Lichen planus
- Fibroepithelial polyp, adenoma
- Melanocytic nevus
- Neoplastic lesions
Normal Anatomic Variants
- "Pink pearly penile papules"
- Vestibular papillae (micropapillomatosis labialis)
- Skin tags (acrochordons)
External Genital Squamous Intraepithelial Lesions (SIL)
- Squamous cell carcinoma in situ
- Bowenoid papulosis
- Erythroplasia of Queyrat
- Bowen’s diseases of the genitalia
Sites for Anogenital Warts
Anogenital warts commonly occur in areas of coital friction. For women, external warts can appear on the vulva, vaginal introitus, perineum, and perianal area; women can develop internal warts involving the vagina, cervix, or anal mucosa. In women, external genital warts are more common than vaginal and cervical warts. Intra-anal warts are seen predominantly in persons with a history of receptive anal intercourse. Perianal and intra-anal warts do not necessarily imply anal intercourse as they may develop secondary to autoinoculation, sexual activity other than anal intercourse, or spread from a nearby genital site. For men, anogenital warts may include external warts on the penis, urethral meatus, scrotum, perineum, perianal area, and anal canal (Figure 6).
Symptoms Associated with Anogenital Warts
Most often, genital warts cause minimal symptoms except for cosmetic concerns.[61] Vulvar warts may cause dyspareunia, pruritus, or bleeding. Vaginal warts are usually asymptomatic, although occasional discharge, bleeding, or obstruction of the birth canal (due to increased wart growth during pregnancy) may occur. Penile warts may cause itching. Persons with urethral meatal warts may experience hematuria or impairment of the urinary stream. Perianal and intra-anal warts are usually asymptomatic but may cause pain, bleeding on defecation, or itching.
Anogenital Warts in Preadolescent Children
Anogenital warts in preadolescent children may be due to sexual abuse, although this condition is not diagnostic for sexual abuse. Their appearance should prompt an evaluation by a clinician with special attention to other sexually transmitted infections (STIs) and social risk factors. Anogenital warts in children may result from vertical transmission, transmission of non-genital HPV types to the genital surface, and possibly fomite transmission.
Cervical High-Grade Squamous Intraepithelial Lesions and Cervical Cancer
Cervical high-grade squamous intraepithelial lesion (HSIL), which encompasses the terminology formerly classified as cervical intraepithelial neoplasia grades 2 and 3 (CIN 2 and CIN 3; further details can be found in the section “Cervical Cancer Screening Tests”), is recognized as a true precursor to invasive cervical cancer. Cervical HSIL dysplasia or cervical cancer may occasionally be apparent on physical examination with visual inspection of the cervix, but typically, the visualization of dysplasia or early cancer requires additional modalities. Cervical cellular abnormalities are usually subclinical, and lesions associated with these abnormalities can be detected by Pap test or colposcopy, with or without biopsy of the lesion. Cervical HSIL may regress spontaneously without treatment. Even high-grade cervical intraepithelial neoplasia (CIN) may regress without treatment, particularly for younger women (21–24 years of age), so treatment recommendations vary according to age at diagnosis.[62]
Anal High-Grade Squamous Intraepithelial Lesions and Anal Cancer
Anal HSIL consists of premalignant cellular changes similar in nature to those seen in cervical HSIL. The diagnosis is made based on biopsy of anal tissue, typically after high-resolution anoscopy (HRA). Patients with anal HSIL most commonly have no symptoms and frequently have a normal physical examination (via standard anoscopy and digital anorectal examination). Some patients do describe anal pain, bleeding, or pruritus.[63] In some cases, physical examination may reveal anal lesions with a wide variety of appearances. Although certain physical examination findings, such as large or fixed lesions, ulceration, or bleeding, are more concerning for anal cancer, it is important to note that such findings do not establish a definitive diagnosis of malignancy. In addition, the lack of symptoms or abnormal findings exclude the possibility of cancer. The roles of biopsy and high-resolution anoscopy are still being evaluated for both screening and diagnosis of anal dysplasia and cancer. Anal HSIL may regress without treatment, particularly in younger persons and those with smaller lesions.[64]
Anogenital Cancers
With progression from precancerous lesions to malignancy, the cervix or anal epithelium may become abnormal upon physical examination, with gross erosion, bleeding, ulcer, or mass. These abnormalities can extend from the cervix to vaginal mucosa or reveal tumor erosion into nearby tissue. Bimanual pelvic examination findings may disclose local metastatic involvement. Anorectal examination (via digital anorectal examination and anoscopy) may reveal an external or internal mass, with or without gross blood from tumor erosion.
Diagnosis and Screening Tests
Anogenital Warts
Although most cases of anogenital warts are diagnosed clinically, confirmation by biopsy may be needed in any of the following situations:[65]
- The lesions are atypical (e.g., pigmented, indurated, affixed to underlying tissue, bleeding, or ulcerated).
- The diagnosis is uncertain.
- The person with the anogenital warts is immunocompromised (including individuals with HIV).
- The lesions do not respond to therapy.
- The lesions worsen during treatment.
Application of acetic acid to suspected wart lesions is not routinely recommended due to its low specificity (many false-positives). External genital warts are not an indication for type-specific HPV DNA testing since this information does not alter the management.[65]
Cervical Dysplasia and Cervical Cancer
The application of 3 to 5% acetic acid (vinegar) and/or Lugol’s iodine to lesions has been used as a bedside screening tool, but is not routinely recommended. Magnification by colposcopy can enhance the detection of cervical dysplasia; histology from a biopsy is used to confirm and stage cervical intraepithelial lesions and to confirm cervical cancer.
Cervical Cancer Screening Tests
Cervical Cytology
The Pap test is the main screening test used to detect cervical cytologic abnormalities. The basic principle of the Pap test is to collect cervical cells and examine these cells under a microscope for any evidence of abnormal morphology. The Pap test requires collecting cells from the external surface of the cervix (ectocervix) and the canal of the cervix (endocervix); obtaining cells from the endocervix is particularly important to evaluate the squamocolumnar junction (transformation zone) region, since this region has the highest risk for development of cervical cancer. Collection devices used include wooden and plastic spatulas for ectocervical samples, and brushes and brooms for endocervical samples. The Pap test can be performed using either the conventional method (sample is collected, smeared on a glass cytology slide, and then fixed with a preservative) or liquid-based tests (the spatula or brush is directly placed in liquid collection medium).[66] The 2021 STI Treatment Guidelines also recommend the following considerations related to performing Pap tests:[67]
- Cervical cytology screening (e.g., Pap test) should not be considered a screening test for sexually transmitted infections.
- Liquid-based cytology is an acceptable alternative to conventional Pap tests, as it has similar test-performance characteristics.
- Ideally, the conventional cytology Pap test should be performed 10 to 20 days after menses, whereas liquid-based Pap testing can be performed at any time during the menstrual cycle.
- If specific sexually transmitted infections other than HPV (e.g., chlamydia or gonorrhea) are identified at the visit, the woman might need to have a repeat Pap test after appropriate treatment for those infections. In most instances (even in the presence of some severe infections), Pap tests will be reported as satisfactory for evaluation, and reliable final reports can be produced without the need to repeat the Pap test after treatment is received.
- The presence of a mucopurulent discharge should not postpone Pap testing. The test can be performed after removal of the discharge with a saline-soaked cotton swab.
- In the presence of cervical friability, liquid-based cytology should be used; conventional Pap testing might need to be deferred in the presence of heavy bleeding until cervicitis is treated.
- The presence of external genital warts is not an indication for more frequent Pap testing.
- The sequence of Pap testing in relation to the collection of other endocervical specimens does not influence Pap test results or their interpretation. In general, vaginal specimens are preferred for chlamydia and gonorrhea screening in women, but in the setting of a pelvic exam, endocervical specimens for STI testing can be collected first.
- Health care facilities that train providers on Pap test collection and employ simple quality assurance measures are more likely to obtain satisfactory test results (as determined by the laboratory).
- Use of instruments designed to obtain samples from the cervical transformation zone (e.g., cytobrushes) improves the accuracy of Pap tests.
HPV Testing
The HPV tests are molecular-based tests that can confirm the presence of HPV by detecting viral DNA or mRNA. In the United States, there are several HPV tests that are FDA-cleared for use, but only for testing of cervical specimens. The HPV tests vary from those that detect only the highest risk oncogenic HPV types (16 and 18) to assays that detect a full array of oncogenic HPV types (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, and 68). The HPV assays that specifically detect oncogenic HPV types are sometimes referred to as high-risk HPV (hrHPV) tests. Primary HPV testing is the term used to describe HPV testing alone (without cytology testing). In the United States, there are two HPV tests FDA-cleared for primary HPV testing and five HPV tests approved for cotesting.[68] In May 2024, the FDA approved two tests for HPV testing that allow for self-collection in a health care setting; a clinical trial is currently recruiting to evaluate self-collection in a home setting compared to a health care setting.[69] The main use for HPV testing is for cervical cancer screening and as a component of follow-up testing in women with abnormal Pap smear results. Note that HPV testing is NOT recommended in the following situations:[67]
- Deciding whether to vaccinate against HPV
- Conducting HPV tests for low-risk (nononcogenic) HPV types (e.g., types 6 and 11)
- Providing care to persons with genital warts or their partners
- Testing persons aged younger than 25 years as part of routine cervical cancer screening
- Testing oral specimens
Cotesting
When HPV testing is performed with cytology (Pap smear), it is referred to as cotesting. Multiple studies have shown that combined Pap and HPV testing, when compared with either test alone, increases the rate of detection of grade 2 or 3 cervical intraepithelial neoplasia.[70,71,72] Cotesting can be performed on the same sample or on separate samples.
Nomenclature for Interpretation of Cervical Cancer Screening Tests
Multiple different types of classification systems have been used to report and describe findings on cervical cancer screening results.[2] The major categories used for interpretation are cytology and histology.
- Cytology: The major systems used for cytologic scoring in the United States are the original Papanicolaou (Pap) scoring system and the more recent Bethesda scoring.
- Pap Scoring System: The Pap scoring system in which severity (I–V) is typically graded based on the degree of cytological atypia (abnormal mitotic figures and changes in nuclear shape and size) and the loss of cervical cell cytoplasmic maturation.
- Bethesda Scoring System: The Bethesda scoring system is the major cervical cytology scoring system used in the United States. The Bethesda classifies squamous precursor lesions as low-grade squamous intraepithelial lesions (LSILs) or high-grade squamous intraepithelial lesions (HSILs). Similar to the Lower Anogenital Squamous Terminology (LAST) histology scoring system, it incorporates LSIL and HSIL, but it also includes the designations negative for intraepithelial lesion and malignancy (NILM) and atypical squamous cells of undetermined significance (ASC-US), for an equivocal abnormality.[73]
- Histology: The two major histology systems used in cervical cancer screening are the cervical intraepithelial neoplasia (CIN) scale and the Lower Anogenital Squamous Terminology (LAST) scale.[2]
- CIN: The CIN scale is used for squamous lesions and is based on the fraction of normal epithelial cells replaced by undifferentiated cells; the CIN categories include CIN1 (formerly called mild dysplasia), CIN2 (previously called moderate dysplasia), and CIN3 (previous terms were severe dysplasia and carcinoma in situ). Lesions that are CIN3 are considered premalignant with a potential to progress to invasive cancer.
- LAST: The LAST scale is also used for squamous lesions, and it consists of a two-tiered system that classifies squamous precursor lesions as low-grade squamous intraepithelial lesions (LSIL) or high-grade squamous intraepithelial lesions (HSIL). Lesions that were previously classified as CIN1 correspond to cervical LSIL, and CIN3 lesions correspond to cervical HSIL. Due to the poor reproducibility of CIN2, the differentiation between LSIL and HSIL is made based on immunohistochemical staining of biomarker p16 (a progression-related biomarker).[74,75] The CIN2 lesions that have a negative p16 staining are downgraded to LSIL, whereas p16-positive CIN2 lesions are considered HSIL. The LAST nomenclature system is preferred as it better reflects the current knowledge of HPV infection biology.
Anal Cancer Detection and Screening Tests
Digital Anorectal Exam (DARE)
The International Anal Neoplasia Society (IANS) defines digital anorectal examination (DARE) as palpation of the entire anal canal and visualization/palpation of the anal margin; the anal margin is the area just inside the anal verge (5 cm area distal to the anal verge).[76] The palpation of the anal canal is performed by inserting a gloved finger (with lubricant) into the anus to gently palpate for abnormalities.[76] DARE is considered an extension of the digital rectal examination (DRE). Performing DARE does not require special training or special equipment other than gloves and lubricant. Note that if anal cytology is planned, it should be performed prior to the digital anorectal examination since lubricant should not be in the anal canal when anal Pap testing is performed.[77,78]
Anal Cytology
Anal cytology is the most widely used and evaluated test for anal cancer screening.[79] Although the same general principles related to cervical Pap testing apply to anal Pap testing, several key aspects of obtaining the clinical sample for the anal Pap should be highlighted.[77,78]
- The person undergoing the testing should receive instructions not to place anything in their anus for at least 24 hours, including avoiding anal enemas or douching.
- Lubricants should not be used when performing the anal Pap.
- The swab used for the anal Pap should be synthetic (rayon or polyester) and moistened with tap water prior to the procedure.
- To collect the anal cytology sample, insert the swab 2 to 3 inches into the anal canal; the swab should then slowly be withdrawn over a period of 15 to 30 seconds while using a spiral motion to sample the anal canal circumference.
- Smear the swab on a glass slide (conventional cytology) or place the swab in liquid media (liquid-based cytology); either of these methods is acceptable when performing anal Pap testing.
Anal HPV Testing
Despite the use of HPV DNA detection as a diagnostic test, there are no FDA-approved assays for anal specimens, requiring individual laboratories to validate the methodologies for this purpose. Anal cancer screening with HPV testing (high-risk HPV types [hrHPV]) alone or in combination with cytology (cotesting) are options for screening.[79] Available data suggest that anal cotesting does not provide benefit over primary hrHPV testing for anal HSIL; in addition, cotesting may be less helpful in populations with a high baseline prevalence of hrHPV.[67]
High-Resolution Anoscopy
High-resolution anoscopy is the process of examining the anal canal and perianal region with a colposcope (to provide lighting and magnification) in conjunction with repeated application of acetic acid and Lugol’s iodine solution (to identify lesions in the anal epithelium) during the procedure.[80] The goal of this office-based procedure is to visualize the entire anal canal and perianal region.[80] High-resolution anoscopy should only be performed by persons who have received adequate professional training in performing this procedure and in performing anal biopsies.[80] Routine use of high-resolution anoscopy as a primary screening tool for anal cancer is not recommended. Programs that perform anal cytology testing should ideally have good access to high-resolution anoscopy for evaluation of persons who have an abnormal anal Pap. High-resolution anoscopy with targeted biopsies of lesions is considered the gold standard for diagnosing anal dysplasia (Figure 7).[67,81,82]
Reporting and Public Health Follow-Up
HPV infection is not reportable in any state.
Screening Recommendations for HPV-Related Cancers
Cervical Cancer Screening
There is ample evidence for the effectiveness of screening for HPV-associated precancers for women. In recent years, multiple organizations have been moving to consolidate and align cervical cancer screening recommendations. To this end, the 2018 United States Preventive Services Task Force (USPSTF) Cervical Cancer Screening Recommendations have now been formally endorsed by the American College of Obstetricians and Gynecologists (ACOG), the Society of Gynecologic Oncology (SGO), and the American Society for Colposcopy and Cervical Pathology.[83]
USPSTF Cervical Cancer Screening Recommendations
The following summarizes key elements in cervical cancer screening recommendations from the 2018 United States Preventive Services Task Force (USPSTF).[84,85] Note the USPSTF gives an “A” rating for cervical cancer screening for women who are 21–65 years of age.[84,85]
- Type of Screening: The cervical cytology (Pap test) screening should be performed using either conventional or liquid-based cytologic tests. The HPV testing should utilize one of several FDA-cleared oncogenic or high-risk HPV tests.
- Age for Conducting Screening: Routine cervical screening should be performed starting at age 21 years and continuing through age 65 years.
- Women Younger than 21 Years of Age: Cervical cancer screening is not recommended for women younger than 21 years of age.
- Women 21 through 29 Years of Age: For women aged 21 through 29 years, cervical cytology screening is recommended every 3 years.
- Women 30 through 65 Years of Age: For women aged 30 through 65 years, cervical cancer screening is recommended and includes three options: (1) cervical cytology alone every 3 years, (2) high-risk HPV testing alone every 5 years, or (3) cervical cytology in combination with high-risk HPV testing every 5 years.
- Women Older than 65 Years of Age: Cervical cancer screening is not recommended in women who are older than 65 years of age who have had adequate prior cervical cancer screening and who are not at high risk of cervical cancer. In certain populations, such as in women with HIV, the recommendation is to continue cervical cancer screening indefinitely.
- Women with Hysterectomy: Cervical cancer screening is not recommended for women who have had a hysterectomy (with removal of the cervix), if they do not have a history of a cervical high-grade squamous intraepithelial lesion or cervical cancer.
- Prior HPV Immunization: Recommendations for cervical screening should not be determined by prior receipt of the HPV vaccine and should follow age-specific screening recommendations.
Table 3. USPSTF Cervical Cancer Screening Recommendations
Population of Women* Recommendation USPSTF Grade# Age <21 years No screening D Age 21-29 years Cytology alone every 3 years^ A Age 30-65 years Any one of the following:
- Cytology alone every 3 years
- FDA-approved primary hrHPV testing every 5 years
- Cotesting (hrHPV testing and cytology) every 5 years
A Age >65 years No screening after adequate negative prior screening results and not otherwise at risk for cervical cancer§ D Hysterectomy with removal of cervix No screening in women who do not have a history of high-grade cervical precancerous lesions (i.e., cervical intraepithelial neoplasia [CIN] grade 2 or 3) or cervical cancer D Abbreviations: FDA = Food and Drug Administration; hrHPV = high-risk human papillomavirus
*Recommendations apply to women with a cervix who do not have signs or symptoms of cervical cancer; recommendations are regardless of sexual history or vaccination status; these recommendations do not apply to women at risk of cervical cancer (e.g., prior diagnosis of high-grade precancerous cervical lesion, women with in utero exposure to diethylstilbestrol, or immunocompromised women)
#Grade A = high certainty; the net benefit is substantial; Grade D = USPSTF recommends against performing this service
^Primary hrHPV testing is approved starting at age 25 years; primary hrHPV testing every 5 years can be considered as an alternative to cytology-only screening in average risk patients aged 25–29 years
§Adequate negative prior test results is defined as three consecutive negative cytology results, two consecutive negative cotesting results, or two negative hrHPV testing results within 10 years before stopping screening, with the most recent test occurring within the recommended screening interval for the test used.
American Cancer Society Cervical Cancer Screening Recommendations
The following summarizes key elements in cervical cancer screening recommendations from the American Cancer Society for women who have a cervix.[68]
- Type of Screening: Screening for cervical cancer should consist of primary HPV testing every 5 years. If primary HPV testing is not available, there are two screening options: (1) cotest with an HPV test and a Pap test every 5 years or (2) a Pap test alone every 3 years. Note that a primary HPV test is considered a standalone HPV test.
- Age for Conducting Screening: Routine cervical screening should be performed starting at age 25 years and continuing through age 65 years.
- Screening for Women 65 Years of Age and Older: Cervical cancer screening is not recommended in women who are older than 65 years of age if they have had screening in the prior 10 years with normal results and no history of CIN2 (or more serious diagnosis) in the past 25 years.
- Women with Prior Complete Hysterectomy: Cervical cancer screening is not recommended for women who have undergone a total hysterectomy (removal of uterus and cervix), unless the procedure was performed for treatment of cervical cancer or serious cervical precancer. In addition, women who previously had a supra-cervical hysterectomy, in which the cervix remains in place, should continue cervical cancer screening using age-based recommendations.
- Women with Prior Precancer: For women previously diagnosed with a cervical precancer, screening should continue for at least 25 years, even if this extends past 65 years of age.
- Screening for Women who are Immunosuppressed: For women who are immunosuppressed, including women with HIV, cervical cancer screening may need to occur more frequently than the recommended intervals.
- Prior HPV Immunization: Recommendations for cervical screening should not be determined by prior receipt of HPV vaccine and should follow age-specific screening recommendations.
Screening for Cervical Cancer in Women who are Pregnant
Screening for cervical cancer in pregnant women should be at the same intervals as nonpregnant women. In this setting, a swab, Ayre’s spatula, or cytobrush can be used for obtaining Pap tests in pregnant women. Abnormal results should be referred to a specialist for discussion of treatment options.
Screening for Cervical Cancer in Women with HIV
Several studies have documented a 3- to 4-fold increased risk of cervical cancer in women with HIV compared with women without HIV.[86,87] Accordingly, cervical cancer screening for women with HIV tends to start at an earlier age, occurs with more frequency, and continues for longer than in women without HIV.[88] The following summarizes the HIV Adult and Adolescent Opportunistic Infection Guidelines recommendations for cervical cancer screening.[88]
- Cervical Cancer Screening at Entry to HIV Care: Women with HIV who are sexually active and at least 21 years of age should undergo cervical cancer screening at initial entry to HIV care and again 12 months later. The screening test used should be determined by the woman’s age.
- Age for Conducting Screening: Women with HIV should receive baseline cervical cancer screening starting at 21 years of age. Cervical cancer screening in women with HIV should continue throughout their lifetime and not end at 65 years of age.
- Women Younger than 30 Years of Age: For women with HIV younger than 30 years of age, cervical cytology screening (Pap test) is recommended. If the initial Pap test is normal, then follow-up Pap testing should be performed in 12 months. If the results of 3 consecutive Pap tests are normal, the interval for follow-up Pap testing should extend to every 3 years. For women younger than 30 years of age, cotesting (Pap test and HPV test) is not recommended.
- Women 30 Years of Age and Older: For women with HIV who are 30 years of age and older, the acceptable screening options are Pap testing alone or cotesting (Pap and HPV). If screening with Pap testing alone, the Pap test should be performed at the time of HIV diagnosis (baseline), then every 12 months. If the results of 3 consecutive Pap tests are normal, then follow-up Pap testing should be every 3 years. If cotesting is done at the time of diagnosis and the results are normal, then the next screening for cervical cancer should be performed in 3 years. Women with a normal Pap test but a positive HPV test should have cotesting repeated in 1 year. If, on repeat testing, cytology is abnormal or any high-risk HPV is detected, then referral for colposcopy is recommended. In addition, if initial HPV testing is performed and is positive for HPV 16 or 16/18, then referral for colposcopy is recommended.
Management of Cervical Cellular Abnormalities
Management of cervical cellular abnormalities is complex and requires synthesis of the woman’s age, Pap test results, high-risk HPV testing, and pathology from any biopsy samples. High-risk HPV DNA cotesting serves primarily to allow safe the deferment of lower-risk lesions and cellular abnormalities of undetermined significance. The approach and management of women with cervical cellular abnormalities is beyond the scope of this lesson, but is addressed in detail in the 2019 American Society for Colposcopy and Cervical Pathology (ASCCP) Risk-Based Management Consensus Guidelines for Abnormal Cervical Cancer Screening Tests and Cancer Precursors.[89] In addition, the approach and management of women with HIV with cervical cellular abnormalities is addressed in the HIV Adult and Adolescent Opportunistic Infection Guidelines.[88]
Screening for Anal Cancer
Anal cancer disproportionately affects certain populations, including persons with HIV, men who have sex with men (MSM), solid organ transplant recipients, and women with a history of cervical (or vulvar) HSIL or cancer.[90] Although evidence is limited on the natural history of anal intraepithelial neoplasia lesions, reliability of screening methods, safety and response to treatments, and programmatic considerations, the Anal Cancer/HSIL Outcomes Research (ANCHOR) study found that treatment of anal HSIL reduced anal cancer risk in people with HIV.[64] This finding, combined with data on the increased risk of anal cancer among other certain groups and acceptable performance from screening modalities, have been foundational for evidence-informed anal cancer screening recommendations.[79]
Screening for Anal Cancer in Persons Without HIV
The International Anal Neoplasia Society (IANS) Consensus Guidelines for Anal Cancer Screening provide anal cancer screening strategies for persons without and with HIV; these recommendations are intended for populations with access to HRA.[79]
- When to Start Screening
- MSM without HIV: Screening should begin at 45 years of age.
- Solid Organ Transplant Recipients: Screening should begin 10 years post-transplant.
- Women with a History of Vulvar Precancer or Cancer: Screening should begin within 1 year of diagnosis of vulvar precancer or cancer.
- Other Populations: Persons aged 45 years or older with a history of cervical/vaginal HSIL or cancer, perianal warts, persistent (defined as greater than 1 year) cervical HPV16, or autoimmune conditions (including but not limited to rheumatoid arthritis, systemic lupus erythematosus, Crohn's disease, ulcerative colitis, or use of systemic steroid therapy) could be considered for screening with shared decision-making if access to HRA is adequate.
- People Who Have Multiple Indications for Screening: If a person meets criteria in multiple categories, screening should begin at the soonest interval.
- Screening Methods
- Screening Modality: The screening modality recommended should consist of anal cytology, hrHPV screening, or anal cytology with hrHPV cotesting.
- Screening When Limited or Absent HRA Availability: If HRA is not available, screening should be limited to DARE. If access to HRA is limited, defined by the IANS as an HRA wait time of greater than 6 months for evaluation of an abnormal screening test, then using hrHPV testing for those with ASC-US or LSIL cytology can help prioritize individuals who need immediate referral; and if negative for hrHPV, can reduce the need for immediate referral to HRA and can be considered acceptable for anal cancer screening.
- Frequency: Screening should occur on a yearly basis.
Screening for Anal Cancer in Persons with HIV
Among people with HIV, MSM are at the highest risk of anal cancer (greater than 70 per 100,000 person-years for individuals with HIV who are 30 to 44 years of age and greater than 100 per 100,000 person-years for individuals with HIV older than 45 years of age.[79] The following recommendations for screening for anal cancer in persons with HIV are based on HIV Adult and Adolescent Opportunistic Infection Guidelines.[88] Note that all persons with HIV should undergo a yearly assessment of anal symptoms (e.g., unexplained itching, anal bleeding, pain or presence of perianal lesions), regardless of age or history of anal intercourse.[88]
- When to Start Screening Persons with HIV
- MSM: Screening should start screening at 35 years of age.
- Women: Start screening at age 45 years of age.
- Screening Methods
- DARE: Annual DARE is recommended in persons who have an indication for screening and in any person who reports anal symptoms.
- Cytology With or Without with hrHPV Cotesting: Screening should be performed using anal cytology alone or with hr-HPV cotesting. Screening using hr-HPV without cytology is not recommended due to insufficient evidence in persons with HIV.
- Screening Based on Access to HRA: Use of anal cytology to identify those who need HRA should only be performed when HRA and HRA-based treatments are available.
- If HRA is available and cytology is obtained for screening, defer DARE until after the anal canal has been swabbed, as the lubricant can potentially interfere with cytology results.
- If HRA is unavailable, then an assessment of anal symptoms and DARE should be performed instead of cytology.
- If HRA access is limited, then individuals with any of the following risk factors should be prioritized: higher-grade cytologic abnormality, HPV16 on HPV genotyping, current tobacco use, age greater than 60 years, longer known duration of HIV, and history of AIDS.
- Frequency: Screening should occur on a yearly basis.
Management of Anal Cellular Abnormalities and Anal Precancers
The approach and management of persons with anal cellular abnormalities and anal precancers (in people without HIV and people with HIV) is beyond the scope of this lesson but is addressed in the [Guidelines] IANS Guidelines for Anal Cancer Screening and HIV Adult and Adolescent Opportunistic Infection Guidelines.[79,88] Access to anal dysplasia specialists and HRA is often limited, so institutions may need to make modifications to the aforementioned recommendations based on local resources.
Screening for Oropharyngeal Cancer
In the United States, routine screening for HPV-associated oropharyngeal cancer in asymptomatic adults is not recommended.[91]
Treatment of Anogenital Warts
Goals of Wart Treatment
The primary goal for the treatment of anogenital warts is the removal of visible warts.[65] Available therapies reduce but do not completely eliminate the risk of HPV transmission. In addition, there are no data that suggest treatment of genital warts impacts the subsequent risk of anogenital HPV-related cancer. Most individuals have fewer than 10 genital warts and a total wart area of less than 1.0 cm2. Complications rarely occur if treatments for anogenital warts are properly employed. Treatment of anogenital warts typically produces a very good clinical response within 3 months.[65] Although appropriate treatment can induce wart-free periods, subsequent recurrences are common, with a 20 to 50% recurrence rate at 3 to 6 months post-treatment.[92] Reappearance of genital warts within the first several months usually indicates recurrence rather than reinfection. If left untreated, visible genital warts persist with or without proliferation, but some regress spontaneously. Because spontaneous resolution of anogenital warts can occur, some individuals may choose to defer treatment and await possible spontaneous resolution.
Selection of Therapy for Anogenital Warts
Among recommended treatments, there is no evidence that any treatment is superior to others.[65] The choice of the specific treatment should depend on the location of anogenital warts, provider treatment experience, available therapies, preference of the person with the anogenital warts, and pregnancy status.[65] For persons desiring treatment of their anogenital warts, the major initial decision point is whether to utilize patient-applied or provider-administered therapy.[65] Although provider-administered therapies often result in more rapid resolution and require fewer treatments, many individuals prefer to self-apply therapy since this can be done in the privacy of their home and without having to make multiple clinic visits.[65] In general, warts with a relatively small area respond to a wide range of patient-applied and provider-administered treatment modalities, whereas treatment options with very large warts are limited, usually requiring provider-administered treatment. For provider-administered options, cryotherapy and surgical removal are feasible in all anatomic locations; trichloroacetic acid (TCA) or bichloroacetic acid (BCA) is acceptable for treatment of vaginal, cervical, and intra-anal warts; and the use of TCA, BCA, or podophyllin is contraindicated for urethral meatus warts.
Therapy for External Anogenital Warts
Multiple patient-applied and provider-administered therapies are recommended as options for the treatment of external anogenital warts.[65] Medical providers should have appropriate knowledge and training for at least one provider-administered and one patient-applied treatment. Some clinicians will initiate therapy with a provider-administered option to make rapid initial progress in the treatment of warts and then transition to patient-applied therapy when the bulk of warts have been significantly reduced. The following summarizes several recommendations for the use of patient-applied and provider-administered therapies for external anogenital warts.[65]
Patient-Applied Therapies
The recommended patient-applied options include imiquimod cream, podofilox (podophyllotoxin) solution or gel, and sinecatechins (green tea extract); all require repeated applications.
- Imiquimod Cream: The imiquimod 5% cream should be applied to the warts 3 times per week at bedtime for up to 16 weeks, whereas the lower-strength imiquimod 3.75% cream requires application every night at bedtime for up to 8 weeks; with either cream, it should be left on the warts for 6-10 hours and then thoroughly washed off with soap and water. Irritation, burning, and pain are potential side effects of this topical treatment.
- Podofilox: The podofilox 0.5% solution or gel should be applied to the warts in weekly cycles of a twice-daily application for 3 days, followed by no treatment for 4 days; the solution should be applied with a cotton swab and the gel with a finger. When using podofilox, it is important that the total volume of podofilox does not exceed 0.5 mL/day and the total wart area treated does not exceed 10 cm2. The podofilox treatments can be given for up to 4 weekly cycles.
- Sinecatechins: The sinecatechins 15% ointment should be administered 3 times/day using a finger to apply a 0.5 cm strand of ointment to each anogenital wart; the goal is to cover the wart entirely with a thin layer of the sinecatechins. The ointment should not be washed off after application. Genital, anal, and oral sexual contact should be avoided while sinecatechins ointment is present on the skin. This treatment can be administered for up to 16 weeks. Treatment with sinecatechins is not recommended for persons with genital herpes or for immunocompromised persons, including those with HIV.
Provider-Administered Therapies
The recommended treatments for anogenital warts administered by a medical provider include cryotherapy, surgical removal, and application of TCA or BCA.
- Cryotherapy: This process uses the application of liquid nitrogen to destroy the anogenital warts via thermal-induced cytolysis. Most clinicians can easily learn how to use cryotherapy for the treatment of external anogenital warts, but appropriate training should include instruction on the appropriate duration of freezing with each treatment. Post-treatment pain and blistering are common.
- Surgical Removal: Only individuals who have received special training on surgical removal of anogenital warts should use this procedure. Multiple techniques can be used, including tangential scissor excision, tangential shave excision, curettage, laser, or electrocautery. Some surgical procedures used for wart removal may aerosolize HPV; in these situations, a respirator and smoke-evacuating electrocautery can be used to minimize risk.[93]
- Trichloroacetic acid (TCA) or Bichloroacetic acid (BCA): The application of TCA or BCA 80-90% solution should only be performed by an individual with training in this application and for the treatment of small lesions. These acid agents destroy wart tissue by causing chemical coagulation of proteins. Only a small amount of the solution should be applied to the wart, and the solution should dry before the patient moves. If too much is applied or the patient experiences pain, sodium bicarbonate (i.e., baking soda) can be applied to neutralize the acid; the sodium bicarbonate is typically applied as a liquid soap preparation or powdered with talc.
Alternative Therapy for External Anogenital Warts
Limited data are available regarding the efficacy of alternative regimens for treating external anogenital warts, but successful treatment has been reported with podophyllin resin, intralesional interferon, photodynamic therapy, and topical cidofovir.[65] Podophyllin resin has been associated with multiple reports of systemic toxicity when this agent was applied to large lesions or when left on for longer periods than recommended.[94] Podophyllin resin might be considered as an alternative under strict adherence to recommended practice, but routine use of this topical agent is not recommended.
Therapy for Internal Anogenital Warts
Internal anogenital warts, including warts located in the urethral meatus, vagina, cervix, or intra-anal region, are complicated to treat and, in many instances, require management or consultation with a specialist.[65] Although cryotherapy for intra-anal warts is listed as an option, many experts would only use cryotherapy for external anogenital warts.[65]
Genital Wart Follow-Up
Since post-treatment recurrences are common in persons with anogenital warts, a follow-up evaluation 3 months after treatment should be offered. Although post-wart treatment follow-up is not mandatory, it provides an opportunity to monitor for complications of therapy, check for recurrent lesions, document the absence of warts if this has occurred, and reinforce education and counseling messages. The presence of genital warts does not alter indications or frequency for cervical cytology screening, but the [Guidelines] IANS Guidelines for Anal Cancer Screening state that for individuals with perianal warts, screening for anal cancer can be considered with shared decision-making, provided there is access to HRA.[79]
Special Management Considerations
Genital Warts During Pregnancy
Genital warts can proliferate rapidly and become more friable during pregnancy. Watchful waiting is acceptable with smaller lesions. During pregnancy, cryotherapy, trichloroacetic acid, bichloroacetic acid, and surgical removal may be safely used.[65] Cytotoxic agents (podophyllin, podofilox, imiquimod) should not be used during pregnancy.[65] Although pregnant women with genital warts have a risk of transmitting HPV to their child during a vaginal birth, cesarean delivery should not be performed solely to prevent transmission to the neonate, since it is unclear whether cesarean delivery prevents respiratory papillomatosis among infants.[65]
Management of Genital Warts in Immunocompromised Patients
The general approach to the treatment of genital warts in persons with HIV is the same as for those without HIV.[65] Persons with HIV, particularly those individuals with advanced immunosuppression, often have larger or more numerous warts that do not respond as well to therapy, and recurrences occur more frequently after treatment. High-grade squamous intraepithelial lesions (HSIL) and invasive cancer arising within the region of a genital wart (or resembling genital warts) are more frequent in immunocompromised patients; therefore, hyperpigmented lesions and lesions that persist despite treatment (especially in the perianal area) should be promptly evaluated by biopsy. The role of genital warts (or irritated post-treatment sites) in HIV transmission has not been well characterized.
Prevention of HPV Infection
Limiting Number of Sex Partners
Abstaining from sexual activity remains the most reliable method for preventing genital HPV infection.[66,68] Individuals can decrease their risk of acquiring HPV infection by limiting their number of sex partners.[65,67]
Condom Use
Consistent use of latex male condoms can reduce the risk of sexual HPV transmission.[3] For newly sexually active women, one study demonstrated consistent use of condoms by the male partner during vaginal intercourse resulted in a 70% reduction in risk of newly acquired cervical or vulvovaginal HPV infection when compared with male partners who used condoms only 5% of the time.[95] In addition, several studies involving sexually active men who have sex with women have shown an approximately 2-fold lower risk of HPV acquisition among those men who always used a condom when compared with those who never used condoms.[96] There are inadequate data to show benefit of condoms in preventing HPV among MSM.
HPV Vaccines
The HPV vaccine is based on recombinant technology that produces L1 major proteins, which self-assemble into viral-like particles (Figure 8).[24] In the United States, three HPV vaccines (2vHPV, 4vHPV, and 9vHPV) have been licensed for use, but the 9vHPV is now the only available HPV vaccine. The 9vHPV, which was FDA-approved in 2014, offers protection against 7 oncogenic HPV types (16, 18, 31, 33, 45, 52, and 58), which account for approximately 80% of cervical cancers, and 2 HPV types (6 and 11) that cause approximately 90% of genital warts.[97] Based on HPV typing data from samples taken from persons with HPV-associated cancers of the vulva, vagina, anus, penis, and oropharynx, the HPV types in 9vHPV overlap tightly with these cancer-causing HPV types.[4] The 9vHPV vaccine has shown excellent safety in females and males.[98,99]
HPV Vaccine Recommendations
The goal of HPV vaccination is to prevent infection with all the HPV types in the 9vHPV vaccine and, therefore, reduce the risk of genital warts and HPV-related cancers. The following summarizes recommendations of the Advisory Committee for Immunization Practices (ACIP) for the use of the 9vHPV vaccine to prevent HPV infection.[100,101,102]
- Age of Immunization and Age Range: The 9vHPV should be administered routinely at age 11 or 12 years (it can start at age 9 years). Individuals who do not receive 9vHPV by age 13 years can receive 9vHPV through age 26 years as a catch-up vaccination. Persons 27 through 45 years of age who have not previously received the HPV vaccine should engage in shared decision-making with their clinician, as the public health benefit of 9vHPV in older individuals is not clear, since many of these individuals have already acquired multiple HPV types.
- Dosing Schedule: For healthy individuals who initiate the vaccination at ages 9 through 14 years, the 2-dose HPV vaccine schedule is recommended (given at 0 and 6 months). Persons who start the series after 15 years of age require the 3-dose series (given at 0, 1–2 months, and 6 months). In addition, the 3-dose series should be used for individuals with immunocompromising conditions.
- Persons with Immunocompromising Conditions: The 3-dose vaccine series should be used for persons with immunocompromising conditions, including HIV, malignant neoplasms, autoimmune disease, B lymphocyte antibody deficiencies, and T lymphocyte complete or partial defects, and receipt of transplantation or immunosuppressive therapy.
- Recommended Minimal Intervals Between Doses: For the 2-dose vaccine series, the ACIP recommends a minimum interval of 5 months. If the second dose is administered too soon, then it should be repeated (at least 5 months after the first dose). For the 3-dose series, the recommended minimal interval is 4 weeks between the first and second doses, 12 weeks between the second and third doses, and 5 months between the first and third doses; if any dose of the vaccine is administered prior to the recommended minimal interval, it should be repeated after another minimum interval has elapsed since the most recent dose.
- Persons with Immunocompromising Conditions: The 3-dose vaccine series should be used for persons with immunocompromising conditions, including HIV, malignant neoplasms, autoimmune disease, B lymphocyte antibody deficiencies, and T lymphocyte complete or partial defects, and receipt of transplantation or immunosuppressive therapy.
- Interrupted Schedule: If the vaccine schedule is interrupted for longer than the recommended dosing interval, the recommendation is to complete the series without repeating any of the doses. Note that the total number of vaccine doses is based on the age when the first dose was given.
- Pregnancy: The HPV vaccine is not recommended for use during pregnancy. If, however, it is inadvertently given to a pregnant woman, no interventions are required. In addition, pregnancy testing is not needed prior to administering the HPV vaccine.
- Persons Who Previously Received an HPV Vaccine Other than 9vHPV: Persons who previously received 2 doses of either 2vHPV or 4vHPV and the series was initiated prior to age 15 are considered adequately vaccinated. The ACIP does not provide a recommendation for or against giving 9vHPV to persons who previously received a recommended vaccine series with 2vHPV or 4vHPV.
Impact of HPV Vaccine on HPV Prevalence
In the United States and in other countries, significant declines in vaccine-targeted HPV strains occurred within a decade of HPV immunization.[103,104,105] The NHANES registry has been used to longitudinally compare prevalence rates of vaccine-targeted strains (HPV 6, 11, 16, and 18) among females 14 to 34 years of age living in the United States.[106] When comparing prevalence rates for vaccine-targeted strains between the pre-vaccine era (2003-2006) and post-vaccine periods (extending to 2015-2018), major declines in HPV prevalence rates were observed, with an overall decrease of 88% among females aged 14–19 years and 81% among those 20–24 years of age; declines in older women 25–34 years of age also occurred but were not as dramatic as in younger females(Figure 9).[107] There are limited HPV prevalence data in males, but one study demonstrated a 59.4% reduction in persistent anal infections with HPV types 6, 11, 16, and 18 among MSM who had received the 4vHPV vaccine.[108] In addition, several countries with HPV vaccination coverage of 50% or greater have shown early evidence of vaccine cross-protection and herd immunity effects that favorably impact males.[109,110,111]
Impact of HPV Vaccine on Anogenital Warts
In the United States, the trends for anogenital wart prevalence vary by age and sex. The initial declines were observed in 2007–2010 among females 15 to 19 years of age, followed by declines during 2009–2010 among females 20 to 24 years of age.[112] A subsequent study that included data out to 2014 showed continued declines in anogenital wart prevalence in women younger than age 25 and a new decline in women 25–29 years of age.[113] These data, taken together, correlate well with expected declines following the introduction of the 4vHPV vaccine in young females in 2006. Several 4vHPV vaccine trials have shown marked reductions in HPV-related anogenital lesions in female and male participants who received the HPV vaccine compared with those who received placebo.[114,115] In addition, data obtained from 27 clinics participating in the STD Surveillance Network showed an overall 47.1% decrease in anogenital warts during 2010-2016, including significant declines among women (62.2%), men who have sex with women (39%), and MSM (53.4%) (Figure 10).[116] In a meta-analysis involving data from high-income countries, the following major decreases were observed in the diagnosis of anogenital warts: 67% among girls 15 to 19 years of age, 54% among women 20 to 24 years of age, 31% among women 25 to 29 years of age, 48% among boys 15 to 19 years of age, and 32% among men 20 to 24 years of age.[111]
Impact of HPV Vaccine on Cervical Dysplasia and Cancer
Because cervical cancer does not typically develop until at least 15 to 20 years after the initial HPV infection and the 4vHPV vaccine was not widely used until after 2006, there are a limited number of studies demonstrating the effect of the HPV vaccine in lowering rates of cervical cancer. Nevertheless, early data from several studies strongly suggest that HPV vaccination markedly reduces the risk for precancers and cancers of the cervix. In one meta-analysis, the authors concluded that after 5 to 9 years of HPV vaccination, CIN2+ detected on cervical screening decreased by 51% among girls aged 15 to 19 years of age and by 31% among women 20 to 24 years of age.[111] An analysis of the New Mexico HPV Pap Registry from 2007 to 2014 showed significant declines in all stages of cervical intraepithelial neoplasia for women 15 to 19 years of age.[117] Data from the CDC HPV-IMPACT Project, a sentinel surveillance project, also demonstrated dramatic declines in cervical precancer incidence from 2008-2012 for women 18 to 20 years of age.[118] Similarly, between 2008 and 2016, cervical precancer rates (specifically of HPV16/18-CIN2+) declined among women ages 20-24.[119] The most robust data on vaccine-related prevention of cervical cancer is from a nationwide Swedish registry that followed 1,672,983 girls and women who were 10 to 30 years of age from 2006 through 2017 and found that participants who had initiated 4vHPV vaccination before the age of 17 years had an 88% lower risk of cervical cancer than participants who had never received the HPV vaccine.[120]
Impact of HPV Vaccine on Anal Cancer
There are limited data on the impact of HPV vaccine on anal dysplasia and anal cancer. In a randomized 4vHPV vaccine trial that enrolled 602 healthy MSM who were 16 to 26 years of age, the rate of grade 2 or 3 anal intraepithelial neoplasia related to infection with HPV types 6, 11, 16, or 18 was 54.2% lower in the vaccine recipients than in participants who received placebo.[108]Counseling and Education
The 2021 STI Treatment Guidelines recommend the following key counseling and education messages for persons diagnosed with HPV infection.[3]
- Anogenital HPV infection is common. It usually infects the anogenital area but can infect other areas, including the mouth and throat. Most sexually active persons get HPV at some time during their lifetime, although most never know it.
- Partners tend to share HPV, and it is not possible to determine which partner transmitted the original infection. Having HPV does not mean that a person or his or her partner is having sex outside the relationship.
- Persons who acquire HPV usually clear the infection spontaneously, meaning that HPV becomes undetectable with no associated health problems.
- If HPV infection persists, genital warts, precancers, and cancers of the cervix, anus, penis, vulva, vagina, head, or neck might develop.
- Discussion of tobacco use and provision of cessation counseling is important because of its contribution to the persistent infection and progression of HPV-related precancers and cancers.
- Many types of HPV are sexually transmitted through anogenital contact, mainly during vaginal and anal sex. In addition, HPV might also be transmitted during oral sex and genital-to-genital contact without penetration. In rare cases, a pregnant woman can transmit HPV to an infant during delivery.
- Treatments are available for the conditions caused by HPV but not for the virus itself.
- Having HPV does not make it harder for a woman to get pregnant or carry a pregnancy to term. However, certain precancers or cancers that HPV can cause, and the surgical procedures needed to treat them can affect a woman’s ability to get pregnant or carry a pregnancy to term.
- No HPV test can determine which HPV infection will become undetectable and which will persist or progress to disease. However, in certain circumstances, HPV tests can determine whether a woman is at increased risk for cervical cancer.
Partner Management
Sex partner evaluation is not necessary for the management of genital warts because there are no data to indicate that reinfection plays a significant role in recurrences. Providing treatment solely for the purpose of preventing future transmission cannot be recommended because the value of treatment in reducing infectivity is not known. Sex partner counseling provides an opportunity for these partners to learn about the implications of having a partner who has genital warts and about their own potential for future disease transmission. Genital warts are highly infectious, so it benefits the partner to be informed and for the couple to use transmission risk-reduction methods such as consistent and correct condom use. Partner counseling also provides an opportunity to offer these partners STI and Pap screening (if appropriate), as well as counseling on prevention. The following are the main counseling issues for sex partners of persons diagnosed with HPV infection.
- Watch for clinical recurrences (most frequently occurring in the first 3 months after treatment).
- Continue regular Pap screening at the same intervals as recommended for women without genital warts.
- Communicate with current sex partners about a current diagnosis of genital warts and the risk of transmission. Patients should have no sexual activity with new partners until the warts are gone or removed.
- Sex partners of persons with genital warts should receive the 9vHPV vaccine if they have not previously received an HPV vaccine (and they are eligible to receive the HPV vaccine).
- Individuals with anogenital warts can still potentially transmit HPV to sex partners after visible warts are gone, since HPV can remain persistent in the tissues.
- The risk of transmitting HPV to sex partners is likely lowered by consistent and correct condom use, but transmission can potentially still occur via contact with areas of skin that cannot be covered with a condom.
Summary Points
- Human papillomavirus (HPV) is one of the most common sexually transmitted infections, with approximately 40 subtypes that can potentially cause anogenital infection. The HPV types are classified based on their oncogenic potential as either low-risk (nononcogenic) types or high-risk types (oncogenic types).
- Low-risk HPV types 6 and 11 cause approximately 90% of genital warts; high-risk HPV types 16 and 18 account for approximately 63% of all HPV-associated cancers and about 70% of cervical cancers; high-risk HPV types 31, 33, 45, 52, and 58 account for an additional 10% of cervical cancers.
- Most HPV infections, whether caused by low-risk or high-risk types, are transient (resolve within 2 years), asymptomatic, and have no clinical consequences.
- Genital warts caused by HPV have four morphologic types: condylomata acuminata, smooth papules, flat papules, and keratotic warts.
- Treatment of anogenital warts includes multiple options, including patient-applied therapies and provider-administered therapies. Since there are no antiviral treatments that eradicate HPV, warts can recur after treatment.
- There is strong evidence to support screening for cervical cancer in women 21 to 65 years of age with cervical Pap testing (and HPV screening in women 30 years of age or older), and several algorithms have been published to guide screening and the management of abnormal results.
- Anal cancer screening recommendations exist for individuals at higher risk for anal cancer, such as MSM with HIV, and are dependent on the ability to access HRA.
- Consistent and correct use of condoms reduces the risk for genital HPV acquisition or transmission but does not entirely prevent transmission of HPV.
- The 9-valent HPV vaccine (9vHPV) is now the only HPV vaccine available in the United States; this vaccine prevents infection with HPV types 6, 11, 16, 18, 31, 33, 45, 52, and 58.
- Use of the HPV vaccines has led to population declines in HPV prevalence, anogenital warts, and HPV-related precancers and cancers.
Check-On-Learning Questions Display Options
These quick questions are meant to keep you on track and check your understanding. They appear throughout the core concepts and are listed here for you to review.Citations
- 1.Doorbar J, Quint W, Banks L, et al. The biology and life-cycle of human papillomaviruses. Vaccine. 2012;30 Suppl 5:F55-70.[PubMed Abstract] -
- 2.Schiffman M, Doorbar J, Wentzensen N, et al. Carcinogenic human papillomavirus infection. Nat Rev Dis Primers. 2016;2:16086.[PubMed Abstract] -
- 3.Workowski KA, Bachmann LH, Chan PA, et al. Sexually transmitted infections treatment guidelines, 2021. Human papillomavirus (HPV) infection. MMWR Recomm Rep. 2021;70(No. RR-4):1-187.
- 4.Saraiya M, Unger ER, Thompson TD, et al. US assessment of HPV types in cancers: implications for current and 9-valent HPV vaccines. J Natl Cancer Inst. 2015;107:djv086.[PubMed Abstract] -
- 5.National Cancer Institute: Surveillance, Epidemiology, and End Result Program (SEER) Cancer Stat Facts: Anal Cancer.
- 6.National Cancer Institute: Surveillance, Epidemiology, and End Result Program (SEER) Cancer Stat Facts: Cervical Cancer.
- 7.National Cancer Institute: Surveillance, Epidemiology, and End Result Program (SEER) Cancer Stat Facts: Oral Cavity and Pharynx Cancer.
- 8.Lewis RM, Laprise JF, Gargano JW, et al. Estimated Prevalence and Incidence of Disease-Associated Human Papillomavirus Types Among 15- to 59-Year-Olds in the United States. Sex Transm Dis. 2021;48:273-7.[PubMed Abstract] -
- 9.Machalek DA, Poynten M, Jin F, et al. Anal human papillomavirus infection and associated neoplastic lesions in men who have sex with men: a systematic review and meta-analysis. Lancet Oncol. 2012;13:487-500.[PubMed Abstract] -
- 10.Lin C, Franceschi S, Clifford GM. Human papillomavirus types from infection to cancer in the anus, according to sex and HIV status: a systematic review and meta-analysis. Lancet Infect Dis. 2018;18:198-206.[PubMed Abstract] -
- 11.Sonawane K, Suk R, Chiao EY, et al. Oral Human Papillomavirus Infection: Differences in Prevalence Between Sexes and Concordance With Genital Human Papillomavirus Infection, NHANES 2011 to 2014. Ann Intern Med. 2017;167:714-24.[PubMed Abstract] -
- 12.Gillison ML, Broutian T, Pickard RK, et al. Prevalence of oral HPV infection in the United States, 2009-2010. JAMA. 2012;307:693-703.[PubMed Abstract] -
- 13.Giuliano AR, Felsher M, Waterboer T, et al. Oral Human Papillomavirus Prevalence and Genotyping Among a Healthy Adult Population in the US. JAMA Otolaryngol Head Neck Surg. 2023;149:783-95.[PubMed Abstract] -
- 14.National Cancer Institute. Surveillance, Epidemiology, and End Results Program.
- 15.Llata E, Stenger M, Bernstein K, et al. Prevalence of genital warts among sexually transmitted disease clinic patients-sexually transmitted disease surveillance network, United States, January 2010 to December 2011. Sex Transm Dis. 2014;41:89-93.[PubMed Abstract] -
- 16.Lechner M, Liu J, Masterson L, Fenton TR. HPV-associated oropharyngeal cancer: epidemiology, molecular biology and clinical management. Nat Rev Clin Oncol. 2022;19:306-27.[PubMed Abstract] -
- 17.Shi R, Devarakonda S, Liu L, Taylor H, Mills G. Factors associated with genital human papillomavirus infection among adult females in the United States, NHANES 2007-2010. BMC Res Notes. 2014;7:544.[PubMed Abstract] -
- 18.Bosch FX, de Sanjosé S. The epidemiology of human papillomavirus infection and cervical cancer. Dis Markers. 2007;23:213-27.[PubMed Abstract] -
- 19.Chelimo C, Wouldes TA, Cameron LD, Elwood JM. Risk factors for and prevention of human papillomaviruses (HPV), genital warts and cervical cancer. J Infect. 2013;66:207-17.[PubMed Abstract] -
- 20.Gillison ML, D'Souza G, Westra W, et al. Distinct risk factor profiles for human papillomavirus type 16-positive and human papillomavirus type 16-negative head and neck cancers. J Natl Cancer Inst. 2008;100:407-20.[PubMed Abstract] -
- 21.Doorbar J. Molecular biology of human papillomavirus infection and cervical cancer. Clin Sci (Lond). 2006;110:525-41.[PubMed Abstract] -
- 22.Sapp M, Day PM. Structure, attachment and entry of polyoma- and papillomaviruses. Virology. 2009;384:400-9.[PubMed Abstract] -
- 23.Buck CB, Day PM, Trus BL. The papillomavirus major capsid protein L1. Virology. 2013;445:169-74.[PubMed Abstract] -
- 24.Schiller JT, Davies P. Delivering on the promise: HPV vaccines and cervical cancer. Nat Rev Microbiol. 2004;2:343-7.[PubMed Abstract] -
- 25.Wang JW, Roden RB. L2, the minor capsid protein of papillomavirus. Virology. 2013;445:175-86.[PubMed Abstract] -
- 26.de Villiers EM. Cross-roads in the classification of papillomaviruses. Virology. 2013;445:2-10.[PubMed Abstract] -
- 27.Bzhalava D, Eklund C, Dillner J. International standardization and classification of human papillomavirus types. Virology. 2015;476:341-4.[PubMed Abstract] -
- 28.Viens LJ, Henley SJ, Watson M, et al. Human papillomavirus-associated cancers - United States, 2008-2012. MMWR Morb Mortal Wkly Rep. 2016;65:661-6.[PubMed Abstract] -
- 29.Garland SM, Steben M, Sings HL, et al. Natural history of genital warts: analysis of the placebo arm of 2 randomized phase III trials of a quadrivalent human papillomavirus (types 6, 11, 16, and 18) vaccine. J Infect Dis. 2009;199:805-14.[PubMed Abstract] -
- 30.McBride AA. Human papillomaviruses: diversity, infection and host interactions. Nat Rev Microbiol. 2022;20:95-108.[PubMed Abstract] -
- 31.Mantovani F, Banks L. The human papillomavirus E6 protein and its contribution to malignant progression. Oncogene. 2001;20:7874-87.[PubMed Abstract] -
- 32.Pang CL, Thierry F. Human papillomavirus proteins as prospective therapeutic targets. Microb Pathog. 2013;58:55-65.[PubMed Abstract] -
- 33.Wangu Z, Hsu KK. Impact of HPV vaccination on anogenital warts and respiratory papillomatosis. Hum Vaccin Immunother. 2016;12:1357-62.[PubMed Abstract] -
- 34.Burchell AN, Tellier PP, Hanley J, Coutlée F, Franco EL. Human papillomavirus infections among couples in new sexual relationships. Epidemiology. 2010;21:31-7.[PubMed Abstract] -
- 35.Burchell AN, Coutlée F, Tellier PP, Hanley J, Franco EL. Genital transmission of human papillomavirus in recently formed heterosexual couples. J Infect Dis. 2011;204:1723-9.[PubMed Abstract] -
- 36.Lam JU, Rebolj M, Dugué PA, Bonde J, von Euler-Chelpin M, Lynge E. Condom use in prevention of Human Papillomavirus infections and cervical neoplasia: systematic review of longitudinal studies. J Med Screen. 2014;21:38-50.[PubMed Abstract] -
- 37.Ryndock EJ, Meyers C. A risk for non-sexual transmission of human papillomavirus? Expert Rev Anti Infect Ther. 2014;12:1165-70.[PubMed Abstract] -
- 38.Sabeena S, Bhat P, Kamath V, Arunkumar G. Possible non-sexual modes of transmission of human papilloma virus. J Obstet Gynaecol Res. 2017;43:429-435.[PubMed Abstract] -
- 39.Maturo SC, Hartnick CJ. Juvenile-onset recurrent respiratory papillomatosis. Adv Otorhinolaryngol. 2012;73:105-8.[PubMed Abstract] -
- 40.Derkay CS, Bluher AE. Update on Recurrent Respiratory Papillomatosis. Otolaryngol Clin North Am. 2019;52:669-79.[PubMed Abstract] -
- 41.Moscicki AB, Darragh TM, Berry-Lawhorn JM, et al. Screening for Anal Cancer in Women. J Low Genit Tract Dis. 2015;19:S27-42.[PubMed Abstract] -
- 42.Simpson S Jr, Blomfield P, Cornall A, Tabrizi SN, Blizzard L, Turner R. Front-to-back & dabbing wiping behaviour post-toilet associated with anal neoplasia & HR-HPV carriage in women with previous HPV-mediated gynaecological neoplasia. Cancer Epidemiol. 2016;42:124-32.[PubMed Abstract] -
- 43.Ho GY, Bierman R, Beardsley L, Chang CJ, Burk RD. Natural history of cervicovaginal papillomavirus infection in young women. N Engl J Med. 1998;338:423-8.[PubMed Abstract] -
- 44.de Sanjosé S, Brotons M, Pavón MA. The natural history of human papillomavirus infection. Best Pract Res Clin Obstet Gynaecol. 2018;47:2-13.[PubMed Abstract] -
- 45.Gravitt PE, Winer RL. Natural History of HPV Infection across the Lifespan: Role of Viral Latency. Viruses. 2017;9:267.[PubMed Abstract] -
- 46.Anic GM, Lee JH, Stockwell H, et al. Incidence and human papillomavirus (HPV) type distribution of genital warts in a multinational cohort of men: the HPV in men study. J Infect Dis. 2011;204:1886-92.[PubMed Abstract] -
- 47.Arima Y, Winer RL, Feng Q, et al. Development of genital warts after incident detection of human papillomavirus infection in young men. J Infect Dis. 2010;202:1181-4.[PubMed Abstract] -
- 48.Winer RL, Kiviat NB, Hughes JP, et al. Development and duration of human papillomavirus lesions, after initial infection. J Infect Dis. 2005;191:731-8.[PubMed Abstract] -
- 49.Insinga RP, Perez G, Wheeler CM, et al. Incidence, duration, and reappearance of type-specific cervical human papillomavirus infections in young women. Cancer Epidemiol Biomarkers Prev. 2010;19:1585-94.[PubMed Abstract] -
- 50.Schiffman M, Kjaer SK. Chapter 2: Natural history of anogenital human papillomavirus infection and neoplasia. J Natl Cancer Inst Monogr. 2003;(31):14-9.[PubMed Abstract] -
- 51.Schiffman M, Solomon D. Clinical practice. Cervical-cancer screening with human papillomavirus and cytologic cotesting. N Engl J Med. 2013;369:2324-31.[PubMed Abstract] -
- 52.Woodman CB, Collins SI, Young LS. The natural history of cervical HPV infection: unresolved issues. Nat Rev Cancer. 2007;7:11-22.[PubMed Abstract] -
- 53.Schiffman M, Wentzensen N. Human papillomavirus infection and the multistage carcinogenesis of cervical cancer. Cancer Epidemiol Biomarkers Prev. 2013;22:553-60.[PubMed Abstract] -
- 54.Moscicki AB, Ma Y, Farhat S, et al. Natural history of anal human papillomavirus infection in heterosexual women and risks associated with persistence. Clin Infect Dis. 2014;58:804-11.[PubMed Abstract] -
- 55.Marra E, Kovaleva A, Bruisten SM, Vermeulen W, Boyd A, Schim van der Loeff MF. Incidence and Clearance of Anal High-risk Human Papillomavirus Infections and Their Determinants Over 5 Years Among Human Immunodeficiency Virus-negative Men Who Have Sex With Men. Clin Infect Dis. 2019;68:1556-65.[PubMed Abstract] -
- 56.Nyitray AG, Carvalho da Silva RJ, Chang M, et al. Incidence, duration, persistence, and factors associated with high-risk anal human papillomavirus persistence among HIV-negative men who have sex with men: a multinational study. Clin Infect Dis. 2016;62:1367-74.[PubMed Abstract] -
- 57.Poynten IM, Jin F, Roberts JM, et al. The Natural history of anal high-grade squamous intraepithelial lesions in gay and bisexual men. Clin Infect Dis. 2021;72:853-61.[PubMed Abstract] -
- 58.Kreimer AR, Pierce Campbell CM, Lin HY, et al. Incidence and clearance of oral human papillomavirus infection in men: the HIM cohort study. Lancet. 2013;382:877-87.[PubMed Abstract] -
- 59.Juckett G, Hartman-Adams H. Human papillomavirus: clinical manifestations and prevention. Am Fam Physician. 2010;82:1209-13.[PubMed Abstract] -
- 60.Van Dyne EA, Henley SJ, Saraiya M, Thomas CC, Markowitz LE, Benard VB. Trends in human papillomavirus-associated cancers - United States, 1999-2015. MMWR Morb Mortal Wkly Rep. 2018;67:918-24.[PubMed Abstract] -
- 61.Gilson R, Nugent D, Werner RN, Ballesteros J, Ross J. 2019 IUSTI-Europe guideline for the management of anogenital warts. J Eur Acad Dermatol Venereol. 2020;34:1644-53.[PubMed Abstract] -
- 62.Massad LS, Einstein MH, Huh WK, et al. 2012 updated consensus guidelines for the management of abnormal cervical cancer screening tests and cancer precursors. Obstet Gynecol. 2013;121:829-46.[PubMed Abstract] -
- 63.Hicks CW, Wick EC, Leeds IL, et al. Patient Symptomatology in Anal Dysplasia. JAMA Surg. 2015;150:563-9.[PubMed Abstract] -
- 64.Palefsky JM, Lee JY, Jay N, et al. Treatment of Anal High-Grade Squamous Intraepithelial Lesions to Prevent Anal Cancer. N Engl J Med. 2022;386:2273-82.[PubMed Abstract] -
- 65.Workowski KA, Bachmann LH, Chan PA, et al. Sexually transmitted infections treatment guidelines, 2021. Human papillomavirus (HPV) infection: anogenital warts. MMWR Recomm Rep. 2021;70(No. RR-4):1-187.
- 66.Marchand L, Mundt M, Klein G, Agarwal SC. Optimal collection technique and devices for a quality pap smear. WMJ. 2005;104:51-5.[PubMed Abstract] -
- 67.Workowski KA, Bachmann LH, Chan PA, et al. Sexually transmitted infections treatment guidelines, 2021. Human papillomavirus (HPV) infection: HPV-associated cancers and precancers. MMWR Recomm Rep. 2021;70(No. RR-4):1-187.
- 68.Fontham ETH, Wolf AMD, Church TR, et al. Cervical cancer screening for individuals at average risk: 2020 guideline update from the American Cancer Society. CA Cancer J Clin. 2020;70:321-46.[PubMed Abstract] -
- 69.National Cancer Institute. FDA Approves HPV Tests That Allow for Self-Collection in a Health Care Setting. July 24, 2024.
- 70.Ronco G, Segnan N, Giorgi-Rossi P, et al. Human papillomavirus testing and liquid-based cytology: results at recruitment from the new technologies for cervical cancer randomized controlled trial. J Natl Cancer Inst. 2006;98:765-74.[PubMed Abstract] -
- 71.Kotaniemi-Talonen L, Nieminen P, Anttila A, Hakama M. Routine cervical screening with primary HPV testing and cytology triage protocol in a randomised setting. Br J Cancer. 2005;93:862-7.[PubMed Abstract] -
- 72.Naucler P, Ryd W, Törnberg S, et al. Human papillomavirus and Papanicolaou tests to screen for cervical cancer. N Engl J Med. 2007;357:1589-97.[PubMed Abstract] -
- 73.Nayar R, Wilbur DC. The Pap Test and Bethesda 2014. "The reports of my demise have been greatly exaggerated." (after a quotation from Mark Twain). Acta Cytol. 2015;59:121-32.[PubMed Abstract] -
- 74.Darragh TM, Colgan TJ, Cox JT, et al. The Lower Anogenital Squamous Terminology Standardization Project for HPV-Associated Lesions: background and consensus recommendations from the College of American Pathologists and the American Society for Colposcopy and Cervical Pathology. Arch Pathol Lab Med. 2012;136:1266-97.[PubMed Abstract] -
- 75.Darragh TM, Colgan TJ, Thomas Cox J, et al. The Lower Anogenital Squamous Terminology Standardization project for HPV-associated lesions: background and consensus recommendations from the College of American Pathologists and the American Society for Colposcopy and Cervical Pathology. Int J Gynecol Pathol. 2013;32:76-115.[PubMed Abstract] -
- 76.Hillman RJ, Berry-Lawhorn JM, Ong JJ, et al. International Anal Neoplasia Society Guidelines for the Practice of Digital Anal Rectal Examination. J Low Genit Tract Dis. 2019;23:138-46.[PubMed Abstract] -
- 77.Anal Cancer Information. University of California at San Francisco.[UCSF] -
- 78.Park IU, Palefsky JM. Evaluation and Management of Anal Intraepithelial Neoplasia in HIV-Negative and HIV-Positive Men Who Have Sex with Men. Curr Infect Dis Rep. 2010;12:126-33.[PubMed Abstract] -
- 79.Stier EA, Clarke MA, Deshmukh AA, et al. International Anal Neoplasia Society's consensus guidelines for anal cancer screening. Int J Cancer. 2024;154:1694-1702.[PubMed Abstract] -
- 80.Hillman RJ, Cuming T, Darragh T, et al. 2016 IANS International Guidelines for Practice Standards in the Detection of Anal Cancer Precursors. J Low Genit Tract Dis. 2016;20:283-91.[PubMed Abstract] -
- 81.Berry JM, Palefsky JM, Jay N, Cheng SC, Darragh TM, Chin-Hong PV. Performance characteristics of anal cytology and human papillomavirus testing in patients with high-resolution anoscopy-guided biopsy of high-grade anal intraepithelial neoplasia. Dis Colon Rectum. 2009;52:239-47.[PubMed Abstract] -
- 82.Gudur A, Shanmuganandamurthy D, Szep Z, Poggio JL. An Update on the Current Role of High Resolution Anoscopy in Patients With Anal Dysplasia. Anticancer Res. 2019;39:17-23.[PubMed Abstract] -
- 83.Committee on Practice Bulletins—Gynecology.. Practice Bulletin No. 168: Cervical Cancer Screening and Prevention. Obstet Gynecol. 2016;128:e111-30.[PubMed Abstract] -
- 84.U.S. Preventive Services Task Force. Cervical Cancer: Screening. August 21, 2018.
- 85.US Preventive Services Task Force, Curry SJ, Krist AH, et al. Screening for Cervical Cancer: US Preventive Services Task Force Recommendation Statement. JAMA. 2018;320:674-686.[PubMed Abstract] -
- 86.Chaturvedi AK, Madeleine MM, Biggar RJ, Engels EA. Risk of human papillomavirus-associated cancers among persons with AIDS. J Natl Cancer Inst. 2009;101:1120-30.[PubMed Abstract] -
- 87.Stier EA, Engels E, Horner MJ, et al. Cervical cancer incidence stratified by age in women with HIV compared with the general population in the United States, 2002-2016. AIDS. 2021;35:1851-6.[PubMed Abstract] -
- 88.Panel on Opportunistic Infections in Adults and Adolescents with HIV. Guidelines for the prevention and treatment of opportunistic infections in adults and adolescents with HIV: recommendations from the Centers for Disease Control and Prevention, the National Institutes of Health, and the HIV Medicine Association of the Infectious Diseases Society of America. Human papillomavirus disease. July 9, 2024.[HIV.gov] -
- 89.Perkins RB, Guido RS, Castle PE, et al. 2019 ASCCP Risk-Based Management Consensus Guidelines for Abnormal Cervical Cancer Screening Tests and Cancer Precursors. J Low Genit Tract Dis. 2020;24:102-131.[PubMed Abstract] -
- 90.Clifford GM, Georges D, Shiels MS, et al. A meta-analysis of anal cancer incidence by risk group: Toward a unified anal cancer risk scale. Int J Cancer. 2021;148:38-47.[PubMed Abstract] -
- 91.Moyer VA. Screening for oral cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2014;160:55-60.[PubMed Abstract] -
- 92.D'Ambrogio A, Yerly S, Sahli R, et al. Human papilloma virus type and recurrence rate after surgical clearance of anal condylomata acuminata. Sex Transm Dis. 2009;36:536-40.[PubMed Abstract] -
- 93.Fox-Lewis A, Allum C, Vokes D, Roberts S. Human papillomavirus and surgical smoke: a systematic review. Occup Environ Med. 2020;77:809-17.[PubMed Abstract] -
- 94.Filley CM, Graff-Richard NR, Lacy JR, Heitner MA, Earnest MP. Neurologic manifestations of podophyllin toxicity. Neurology. 1982;32:308-11.[PubMed Abstract] -
- 95.Winer RL, Hughes JP, Feng Q, et al. Condom use and the risk of genital human papillomavirus infection in young women. N Engl J Med. 2006;354:2645-54.[PubMed Abstract] -
- 96.Pierce Campbell CM, Lin HY, Fulp W, et al. Consistent condom use reduces the genital human papillomavirus burden among high-risk men: the HPV infection in men study. J Infect Dis. 2013;208:373-84.[PubMed Abstract] -
- 97.Petrosky E, Bocchini JA Jr, Hariri S, et al. Use of 9-valent human papillomavirus (HPV) vaccine: updated HPV vaccination recommendations of the advisory committee on immunization practices. MMWR Morb Mortal Wkly Rep. 2015;64:300-4.[PubMed Abstract] -
- 98.Moreira ED Jr, Block SL, Ferris D, et al. Safety Profile of the 9-Valent HPV Vaccine: A Combined Analysis of 7 Phase III Clinical Trials. Pediatrics. 2016;138:pii:e20154387.[PubMed Abstract] -
- 99.Markowitz LE, Gee J, Chesson H, Stokley S. Ten years of human papillomavirus vaccination in the United States. Acad Pediatr. 2018;18:S3-S10.[PubMed Abstract] -
- 100.Advisory Committee on Immunization Practices (ACIP). Recommended Child and Adolescent Immunization Schedule for ages 18 years or younger, United States, 2025[ACIP] -
- 101.Advisory Committee on Immunization Practices (ACIP). Recommended Immunization Schedule for Ages 19 Years or Older, United States, 2025.[ACIP] -
- 102.Meites E, Szilagyi PG, Chesson HW, Unger ER, Romero JR, Markowitz LE. Human Papillomavirus Vaccination for Adults: Updated Recommendations of the Advisory Committee on Immunization Practices. MMWR Morb Mortal Wkly Rep. 2019;68:698-702.[PubMed Abstract] -
- 103.Machalek DA, Garland SM, Brotherton JML, et al. Very low prevalence of vaccine human papillomavirus types among 18- to 35-year old Australian women 9 Years following implementation of vaccination. J Infect Dis. 2018;217:1590-1600.[PubMed Abstract] -
- 104.Joura EA, Giuliano AR, Iversen OE, et al. A 9-valent HPV vaccine against infection and intraepithelial neoplasia in women. N Engl J Med. 2015;372:711-23.[PubMed Abstract] -
- 105.Dunne EF, Naleway A, Smith N, et al. Reduction in Human Papillomavirus Vaccine Type Prevalence Among Young Women Screened for Cervical Cancer in an Integrated US Healthcare Delivery System in 2007 and 2012-2013. J Infect Dis. 2015;212:1970-5.[PubMed Abstract] -
- 106.Markowitz LE, Liu G, Hariri S, Steinau M, Dunne EF, Unger ER. Prevalence of HPV After Introduction of the Vaccination Program in the United States. Pediatrics. 2016;137:e20151968.[PubMed Abstract] -
- 107.Rosenblum HG, Lewis RM, Gargano JW, Querec TD, Unger ER, Markowitz LE. Declines in Prevalence of Human Papillomavirus Vaccine-Type Infection Among Females after Introduction of Vaccine - United States, 2003-2018. MMWR Morb Mortal Wkly Rep. 2021;70:415-20.[PubMed Abstract] -
- 108.Palefsky JM, Giuliano AR, Goldstone S, et al. HPV vaccine against anal HPV infection and anal intraepithelial neoplasia. N Engl J Med. 2011;365:1576-85.[PubMed Abstract] -
- 109.Drolet M, Bénard É, Boily MC, et al. Population-level impact and herd effects following human papillomavirus vaccination programmes: a systematic review and meta-analysis. Lancet Infect Dis. 2015;15:565-80.[PubMed Abstract] -
- 110.Chow EP, Machalek DA, Tabrizi SN, et al. Quadrivalent vaccine-targeted human papillomavirus genotypes in heterosexual men after the Australian female human papillomavirus vaccination programme: a retrospective observational study. Lancet Infect Dis. 2017;17:68-77.[PubMed Abstract] -
- 111.Drolet M, Bénard É, Pérez N, Brisson M. Population-level impact and herd effects following the introduction of human papillomavirus vaccination programmes: updated systematic review and meta-analysis. Lancet. 2019;394:497-509.[PubMed Abstract] -
- 112.Flagg EW, Schwartz R, Weinstock H. Prevalence of anogenital warts among participants in private health plans in the United States, 2003-2010: potential impact of human papillomavirus vaccination. Am J Public Health. 2013;103:1428-35.[PubMed Abstract] -
- 113.Flagg EW, Torrone EA. Declines in Anogenital Warts Among Age Groups Most Likely to Be Impacted by Human Papillomavirus Vaccination, United States, 2006-2014. Am J Public Health. 2018;108:112-9.[PubMed Abstract] -
- 114.Garland SM, Hernandez-Avila M, Wheeler CM, et al. Quadrivalent vaccine against human papillomavirus to prevent anogenital diseases. N Engl J Med. 2007;356:1928-43.[PubMed Abstract] -
- 115.Giuliano AR, Palefsky JM, Goldstone S, et al. Efficacy of quadrivalent HPV vaccine against HPV Infection and disease in males. N Engl J Med. 2011;364:401-11.[PubMed Abstract] -
- 116.Mann LM, Llata E, Flagg EW, et al. Trends in the prevalence of anogenital warts among patients at sexually transmitted disease cinics-Sexually Transmitted Disease Surveillance Network, United States, 2010-2016. J Infect Dis. 2019;219:1389-97.[PubMed Abstract] -
- 117.Benard VB, Castle PE, Jenison SA, et al. Population-Based Incidence Rates of Cervical Intraepithelial Neoplasia in the Human Papillomavirus Vaccine Era. JAMA Oncol. 2017;3:833-7.[PubMed Abstract] -
- 118.Hariri S, Johnson ML, Bennett NM, et al. Population-based trends in high-grade cervical lesions in the early human papillomavirus vaccine era in the United States. Cancer. 2015;121:2775-81.[PubMed Abstract] -
- 119.Gargano JW, McClung N, Lewis RM, et al. HPV type-specific trends in cervical precancers in the United States, 2008 to 2016. Int J Cancer. 2023;152:137-50.[PubMed Abstract] -
- 120.Lei J, Ploner A, Elfström KM, et al. HPV Vaccination and the risk of invasive cervical cancer. N Engl J Med. 2020;383:1340-8.[PubMed Abstract] -
Additional References
- Bertolotti A, Dupin N, Bouscarat F, Milpied B, Derancourt C. Cryotherapy to treat anogenital warts in nonimmunocompromised adults: Systematic review and meta-analysis. J Am Acad Dermatol. 2017;77:518-526.[PubMed Abstract] -
- Chesson HW, Spicknall IH, Bingham A, et al. The Estimated Direct Lifetime Medical Costs of Sexually Transmitted Infections Acquired in the United States in 2018. Sex Transm Dis. 2021;48:215-21.[PubMed Abstract] -
- Cohen PA, Jhingran A, Oaknin A, Denny L. Cervical cancer. Lancet. 2019;393:169-182.[PubMed Abstract] -
- Garland SM, Cheung TH, McNeill S, et al. Safety and immunogenicity of a 9-valent HPV vaccine in females 12-26 years of age who previously received the quadrivalent HPV vaccine. Vaccine. 2015;33:6855-64.[PubMed Abstract] -
- Giuliano AR, Isaacs-Soriano K, Torres BN, et al. Immunogenicity and safety of Gardasil among mid-adult aged men (27-45 years)--The MAM Study. Vaccine. 2015;33:5640-6.[PubMed Abstract] -
- Giuliano AR, Lee JH, Fulp W, et al. Incidence and clearance of genital human papillomavirus infection in men (HIM): a cohort study. Lancet. 2011;377:932-40.[PubMed Abstract] -
- Iversen OE, Miranda MJ, Ulied A, et al. Immunogenicity of the 9-Valent HPV Vaccine Using 2-Dose Regimens in Girls and Boys vs a 3-Dose Regimen in Women. JAMA. 2016;316:2411-2421.[PubMed Abstract] -
- Kreuter A, Siorokos C, Oellig F, Silling S, Pfister H, Wieland U. High-grade Dysplasia in Anogenital Warts of HIV-Positive Men. JAMA Dermatol. 2016;152:1225-30.[PubMed Abstract] -
- Lipkind HS, Vazquez-Benitez G, Nordin JD, et al. Maternal and Infant Outcomes After Human Papillomavirus Vaccination in the Periconceptional Period or During Pregnancy. Obstet Gynecol. 2017;130:599-608.[PubMed Abstract] -
- Mayrand MH, Duarte-Franco E, Rodrigues I, et al. Human papillomavirus DNA versus Papanicolaou screening tests for cervical cancer. N Engl J Med. 2007;357:1579-88.[PubMed Abstract] -
- Melnikow J, Henderson JT, Burda BU, Senger CA, Durbin S, Weyrich MS. Screening for Cervical Cancer With High-Risk Human Papillomavirus Testing: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA. 2018;320:687-705.[PubMed Abstract] -
- Mix JM, Van Dyne EA, Saraiya M, Hallowell BD, Thomas CC. Assessing Impact of HPV Vaccination on Cervical Cancer Incidence among Women Aged 15-29 Years in the United States, 1999-2017: An Ecologic Study. Cancer Epidemiol Biomarkers Prev. 2021;30:30-7.[PubMed Abstract] -
- Ong JJ, Grulich A, Walker S, et al. Baseline findings from the Anal Cancer Examination (ACE) study: screening using digital ano-rectal examination in HIV-positive men who have sex with men. J Med Screen. 2016;23:70-6.[PubMed Abstract] -
- Saliba M, Ghossein R, Xu B. HPV-related head and neck cancers: Pathology and biology. J Surg Oncol. 2021;124:923-30.[PubMed Abstract] -
Figures
 Figure 1. Percentage of Urogenital and Oropharyngeal Cancers Caused by HPVSource: Saraiya M, Unger ER, Thompson TD, et al. US assessment of HPV types in cancers: implications for current and 9-valent HPV vaccines. J Natl Cancer Inst. 2015;107:djv086.
Figure 1. Percentage of Urogenital and Oropharyngeal Cancers Caused by HPVSource: Saraiya M, Unger ER, Thompson TD, et al. US assessment of HPV types in cancers: implications for current and 9-valent HPV vaccines. J Natl Cancer Inst. 2015;107:djv086. Figure 2. Estimated HPV Incidence for Persons Aged 15-59 Years, United States, 2018Any HPV = any of 37 types detected using Linear Array; IARC Group 1 = Twelve HPV types are defined by the International Agency for Research on Cancer (IARC) as carcinogenic to humans (HPV 16/18/31/33/35/39/45/51/52/56/58/59); HPV 6/11 = noncarcinogenic HPV types that cause most genital wartsSource: Lewis RM, Laprise JF, Gargano JW, et al. Estimated Prevalence and Incidence of Disease-Associated Human Papillomavirus Types Among 15- to 59-Year-Olds in the United States. Sex Transm Dis. 2021;48:273-7.
Figure 2. Estimated HPV Incidence for Persons Aged 15-59 Years, United States, 2018Any HPV = any of 37 types detected using Linear Array; IARC Group 1 = Twelve HPV types are defined by the International Agency for Research on Cancer (IARC) as carcinogenic to humans (HPV 16/18/31/33/35/39/45/51/52/56/58/59); HPV 6/11 = noncarcinogenic HPV types that cause most genital wartsSource: Lewis RM, Laprise JF, Gargano JW, et al. Estimated Prevalence and Incidence of Disease-Associated Human Papillomavirus Types Among 15- to 59-Year-Olds in the United States. Sex Transm Dis. 2021;48:273-7. Figure 3. Estimated HPV Prevalence for Persons Aged 15-59 Years, United States, 2013-2016Any HPV = any of 37 types detected using Linear Array; IARC Group 1 = Twelve HPV types are defined by the International Agency for Research on Cancer (IARC) as carcinogenic to humans (HPV 16/18/31/33/35/39/45/51/52/56/58/59); HPV 6/11 = noncarcinogenic HPV types that cause most genital wartsSource: Lewis RM, Laprise JF, Gargano JW, et al. Estimated Prevalence and Incidence of Disease-Associated Human Papillomavirus Types Among 15- to 59-Year-Olds in the United States. Sex Transm Dis. 2021;48:273-7.
Figure 3. Estimated HPV Prevalence for Persons Aged 15-59 Years, United States, 2013-2016Any HPV = any of 37 types detected using Linear Array; IARC Group 1 = Twelve HPV types are defined by the International Agency for Research on Cancer (IARC) as carcinogenic to humans (HPV 16/18/31/33/35/39/45/51/52/56/58/59); HPV 6/11 = noncarcinogenic HPV types that cause most genital wartsSource: Lewis RM, Laprise JF, Gargano JW, et al. Estimated Prevalence and Incidence of Disease-Associated Human Papillomavirus Types Among 15- to 59-Year-Olds in the United States. Sex Transm Dis. 2021;48:273-7. Figure 4 (Image Series). Human PapillomavirusHuman papillomavirus is a small, nonenveloped, double-stranded DNA virus that is approximately 55 nm in diameter. The virus has a nonenveloped icosahedral shell primarily consisting of 360 molecules of the L1 major capsid protein arranged as a cluster of 72-pentameric capsomeres.Illustration by 306/Shutterstock.com. Image used under license from Shutterstock.com.
Figure 4 (Image Series). Human PapillomavirusHuman papillomavirus is a small, nonenveloped, double-stranded DNA virus that is approximately 55 nm in diameter. The virus has a nonenveloped icosahedral shell primarily consisting of 360 molecules of the L1 major capsid protein arranged as a cluster of 72-pentameric capsomeres.Illustration by 306/Shutterstock.com. Image used under license from Shutterstock.com. Figure 4B. Human papillomavirus (HPV) Capsid PentamersThis illustration shows the structure of the HPV capsid is based on cryoelectron microscopy. The virus contains 72 pentamers (also referred to as capsomeres), including 12 capsomeres (orange) that are surrounded by five other capsomeres, and 60 capsomeres (red) that are surrounded by six other capsomeres.Source: Goodsell DS. Human Papillomavirus and Vaccines, Protein Data Bank-101.
Figure 4B. Human papillomavirus (HPV) Capsid PentamersThis illustration shows the structure of the HPV capsid is based on cryoelectron microscopy. The virus contains 72 pentamers (also referred to as capsomeres), including 12 capsomeres (orange) that are surrounded by five other capsomeres, and 60 capsomeres (red) that are surrounded by six other capsomeres.Source: Goodsell DS. Human Papillomavirus and Vaccines, Protein Data Bank-101. Figure 4C. Human Papillomavirus L1 Pentameric CapsomereThis illustration shows human papillomavirus (HPV) pentameric capsomere which consists of five L1 proteins. Each HPV capsid contains 360 L1 proteins, which are organized as 72 pentameric capsomeres.Illustration by Leonid Andropov/Shutterstock.com. Image used under license from Shutterstock.com.
Figure 4C. Human Papillomavirus L1 Pentameric CapsomereThis illustration shows human papillomavirus (HPV) pentameric capsomere which consists of five L1 proteins. Each HPV capsid contains 360 L1 proteins, which are organized as 72 pentameric capsomeres.Illustration by Leonid Andropov/Shutterstock.com. Image used under license from Shutterstock.com. Figure 5. Age at Peak Prevalence for Each Stage in Cervical CarcinogenesisNatural history of HPV infection and cancer as shown at top. The bottom graph shows the correlation of the stages during the natural history with age. As shown in the graph, the age of peak high-grade squamous intraepithelial lesions (HSILs) or precancer occurs 5 to 10 years after HPV infection.Source: Schiffman M, Solomon D. Clinical practice. Cervical-cancer screening with human papillomavirus and cytologic cotesting. N Engl J Med. 2013;369:2324-31. © 2013 Massachusetts Medical Society. Reproduced with permission.
Figure 5. Age at Peak Prevalence for Each Stage in Cervical CarcinogenesisNatural history of HPV infection and cancer as shown at top. The bottom graph shows the correlation of the stages during the natural history with age. As shown in the graph, the age of peak high-grade squamous intraepithelial lesions (HSILs) or precancer occurs 5 to 10 years after HPV infection.Source: Schiffman M, Solomon D. Clinical practice. Cervical-cancer screening with human papillomavirus and cytologic cotesting. N Engl J Med. 2013;369:2324-31. © 2013 Massachusetts Medical Society. Reproduced with permission. Figure 6 (Image Series). Genital WartsSource: photograph by Claire Stevens, PA Public Health—Seattle & King County Sexual Health Clinic
Figure 6 (Image Series). Genital WartsSource: photograph by Claire Stevens, PA Public Health—Seattle & King County Sexual Health Clinic Figure 6B. Perineal Warts in a ManThis image shows extensive warts at the base of the scrotum and perianal region.Source: photograph from Public Health—Seattle & King County Sexual Health Clinic
Figure 6B. Perineal Warts in a ManThis image shows extensive warts at the base of the scrotum and perianal region.Source: photograph from Public Health—Seattle & King County Sexual Health Clinic Figure 6C. Perianal CondylomataThis image shows extensive perianal condylomas.Photograph from Jeffrey T. Schouten, M.D., AAHIVEDepartments of Surgery and Medicine, Division of Allergy and Infectious Diseases University of Washington
Figure 6C. Perianal CondylomataThis image shows extensive perianal condylomas.Photograph from Jeffrey T. Schouten, M.D., AAHIVEDepartments of Surgery and Medicine, Division of Allergy and Infectious Diseases University of Washington Figure 6D. Large Intra-Anal CondylomaThis image shows a large, pedunculated lesion seen in anal canal during anoscopy.Photograph from Jeffrey T. Schouten, M.D., AAHIVE Departments of Surgery and Medicine, Division of Allergy and Infectious Diseases University of Washington
Figure 6D. Large Intra-Anal CondylomaThis image shows a large, pedunculated lesion seen in anal canal during anoscopy.Photograph from Jeffrey T. Schouten, M.D., AAHIVE Departments of Surgery and Medicine, Division of Allergy and Infectious Diseases University of Washington Figure 7. Perinanal High-Grade squamous Intraepithelial Lesion (HSIL)Image showing a perianal high-grade squamous intraepithelial lesion (HSIL). Photo A shows small, superficial ulcerative lesion near to the anal verge (black circle). Photo B shows a magnified view of the same lesion using high-resolution anoscopy and acetic acid (black arrow).Photographs from Helen Stankiewicz Karita, M.D., Division of Allergy and Infectious Diseases, University of Washington
Figure 7. Perinanal High-Grade squamous Intraepithelial Lesion (HSIL)Image showing a perianal high-grade squamous intraepithelial lesion (HSIL). Photo A shows small, superficial ulcerative lesion near to the anal verge (black circle). Photo B shows a magnified view of the same lesion using high-resolution anoscopy and acetic acid (black arrow).Photographs from Helen Stankiewicz Karita, M.D., Division of Allergy and Infectious Diseases, University of Washington Figure 8. Human Papillomavirus Vaccine ProductionConceptual rendition of production of human papillomavirus vaccine. The vaccine process involves recombinant synthesis of major capsid L1 proteins that self-assemble as a shell of 72 pentameric capsomeres to form viral-like particles (VLPs). The assembled pseudovirus is very similar to the native human papillomavirus and is highly immunogenic.Illustration: David H. Spach, MD
Figure 8. Human Papillomavirus Vaccine ProductionConceptual rendition of production of human papillomavirus vaccine. The vaccine process involves recombinant synthesis of major capsid L1 proteins that self-assemble as a shell of 72 pentameric capsomeres to form viral-like particles (VLPs). The assembled pseudovirus is very similar to the native human papillomavirus and is highly immunogenic.Illustration: David H. Spach, MD Figure 9. Prevalence of 4vHPV Types among Females Aged 14–34 Years, by Age Group, NHANES, United StatesNHANES = National Health and Nutrition Examination SurveySource: Rosenblum HG, Lewis RM, Gargano JW, Querec TD, Unger ER, Markowitz LE. Declines in Prevalence of Human Papillomavirus Vaccine-Type Infection Among Females after Introduction of Vaccine - United States, 2003-2018. MMWR Morb Mortal Wkly Rep. 2021;70:415-20.
Figure 9. Prevalence of 4vHPV Types among Females Aged 14–34 Years, by Age Group, NHANES, United StatesNHANES = National Health and Nutrition Examination SurveySource: Rosenblum HG, Lewis RM, Gargano JW, Querec TD, Unger ER, Markowitz LE. Declines in Prevalence of Human Papillomavirus Vaccine-Type Infection Among Females after Introduction of Vaccine - United States, 2003-2018. MMWR Morb Mortal Wkly Rep. 2021;70:415-20. Figure 10. Trends in Prevalence of Anogenital Warts, U.S. Sexually Transmitted Disease Surveillance Network, 2010–2016Source: Mann LM, Llata E, Flagg EW, et al. Trends in the prevalence of anogenital warts among patients at sexually transmitted disease cinics-Sexually Transmitted Disease Surveillance Network, United States, 2010-2016. J Infect Dis. 2019;219:1389-97.
Figure 10. Trends in Prevalence of Anogenital Warts, U.S. Sexually Transmitted Disease Surveillance Network, 2010–2016Source: Mann LM, Llata E, Flagg EW, et al. Trends in the prevalence of anogenital warts among patients at sexually transmitted disease cinics-Sexually Transmitted Disease Surveillance Network, United States, 2010-2016. J Infect Dis. 2019;219:1389-97.Tables
Table 1. Human Papillomavirus Types
Low-Risk Types (nononcogenic)
- Associated with genital warts and benign or low-grade cellular changes (mild Pap test abnormalities).
- Approximately 90% of genital warts are caused by HPV types 6 and 11.
- The HPV types causing genital warts can occasionally cause lesions on oral, upper respiratory, upper gastrointestinal, and ocular locations. Recurrent respiratory papillomatosis, a rare condition, is usually associated with HPV types 6 and 11.
High-Risk Types (oncogenic)
- Associated with low-grade cervical cellular changes, high-grade cervical cellular changes (mild, moderate, and severe Pap test abnormalities), cervical dysplasia, and cervical cancer. In addition, associated with cancers of the oropharynx, anus, vulva, vagina, and penis.
- HPV types 16 and 18 account for approximately 65-70% of cervical cancers.
- The HPV types 31, 33, 45, 52, and 58 cause approximately 10% of all HPV-associated cancers.
Table 2. Differential Diagnoses for Anogenital Warts
Manifestations of Other Genital Infections
- Condylomata lata (manifestation of secondary syphilis)
- Molluscum contagiosum
- Herpes vegetans
Acquired Dermatologic Conditions
- Seborrheic keratosis
- Lichen planus
- Fibroepithelial polyp, adenoma
- Melanocytic nevus
- Neoplastic lesions
Normal Anatomic Variants
- "Pink pearly penile papules"
- Vestibular papillae (micropapillomatosis labialis)
- Skin tags (acrochordons)
External Genital Squamous Intraepithelial Lesions (SIL)
- Squamous cell carcinoma in situ
- Bowenoid papulosis
- Erythroplasia of Queyrat
- Bowen’s diseases of the genitalia
Table 3. USPSTF Cervical Cancer Screening Recommendations
Population of Women* Recommendation USPSTF Grade# Age <21 years No screening D Age 21-29 years Cytology alone every 3 years^ A Age 30-65 years Any one of the following:
- Cytology alone every 3 years
- FDA-approved primary hrHPV testing every 5 years
- Cotesting (hrHPV testing and cytology) every 5 years
A Age >65 years No screening after adequate negative prior screening results and not otherwise at risk for cervical cancer§ D Hysterectomy with removal of cervix No screening in women who do not have a history of high-grade cervical precancerous lesions (i.e., cervical intraepithelial neoplasia [CIN] grade 2 or 3) or cervical cancer D Abbreviations: FDA = Food and Drug Administration; hrHPV = high-risk human papillomavirus
*Recommendations apply to women with a cervix who do not have signs or symptoms of cervical cancer; recommendations are regardless of sexual history or vaccination status; these recommendations do not apply to women at risk of cervical cancer (e.g., prior diagnosis of high-grade precancerous cervical lesion, women with in utero exposure to diethylstilbestrol, or immunocompromised women)
#Grade A = high certainty; the net benefit is substantial; Grade D = USPSTF recommends against performing this service
^Primary hrHPV testing is approved starting at age 25 years; primary hrHPV testing every 5 years can be considered as an alternative to cytology-only screening in average risk patients aged 25–29 years
§Adequate negative prior test results is defined as three consecutive negative cytology results, two consecutive negative cotesting results, or two negative hrHPV testing results within 10 years before stopping screening, with the most recent test occurring within the recommended screening interval for the test used.
Table 4. 2021 STI Treatment Guidelines: Anogenital WartsTreatment of External Anogenital WartsExternal anogenital warts include penis, groin, scrotum, vulva, perineum, external anus, and perianus*Recommended for PATIENT-APPLIED TherapyImiquimod 3.75% creamApply the 3.75% cream once at bedtime, every night consecutively for up to 8 weeks.Imiquimod 3.75% cream
Tradename:ZyclaraThe treatment area should be washed with soap and water 6-10 hours after the application.Note: The imiquimod cream might weaken condoms and vaginal diaphragms.Recommended for PATIENT-APPLIED TherapyImiquimod 5% creamApply the 5% cream once at bedtime, three times a week for up to 16 weeks.Imiquimod 5% cream
Tradename:AldaraThe treatment area should be washed with soap and water 6-10 hours after the application.Note: The imiquimod cream might weaken condoms and vaginal diaphragms.Recommended for PATIENT-APPLIED TherapyPodofilox 0.5% solution or gelApply podofilox solution (using a cotton swab) or podofilox gel (using a finger) to anogenital warts twice a day for 3 days, followed by 4 days of no therapy. Repeat the cycle, as necessary, for up to four cycles.Podofilox 0.5% solution or gel
Tradename:CondyloxThe total wart area treated should not exceed 10 cm2, and the total volume of podofilox should be limited to 0.5 mL per day.Recommended for PATIENT-APPLIED TherapySinecatechins 15% ointmentApply three times daily (0.5 cm strand of ointment to each wart) using a finger to ensure coverage with a thin layer of ointment until complete clearance of warts is achieved. This product should not be continued for longer than 16 weeks.Sinecatechins 15% ointment
Tradename:VeregenDo not wash off after use.Note: Sinecatechins might weaken condoms and vaginal diaphragms.Recommended for PROVIDER-ADMINISTERED TherapyCryotherapy with liquid nitrogen or cryoprobeLocal anesthesia (topical or injected) might facilitate therapy if warts are present in many areas or if the area of warts is large.Cryotherapy with liquid nitrogen or cryoprobe
Tradename:Note: Health care providers should be trained on the proper use of this therapy because over- and under-treatment can result in complications or low efficacy.Recommended for PROVIDER-ADMINISTERED TherapySurgical removal either by tangential scissor excision, tangential shaveAfter local anesthesia is applied, anogenital warts can be physically destroyed by electrocautery, in which case no additional hemostasis is required. Alternatively, the warts can be removed either by tangential excision with a pair of fine scissors or a scalpel, by carbon dioxide (CO2) laser, or by curettage.Surgical removal either by tangential scissor excision, tangential shave
Tradename:Note: Surgical therapy has the advantage of eliminating most warts at a single visit, although recurrence can occur. Surgical removal requires substantial clinical training, additional equipment, and sometimes a longer office visit.Recommended for PROVIDER-ADMINISTERED TherapyTrichloroacetic acid (TCA) or Bichloroacetic acid (BCA) 80-90% solutionA small amount should be applied only to the warts and allowed to dry (i.e. develop white frost on tissue) before the patient sits or stands.Trichloroacetic acid (TCA) or Bichloroacetic acid (BCA) 80-90% solution
Tradename:If pain is intense or an excess amount of acid is applied, the area can be covered with sodium bicarbonate (i.e., baking soda), washed with liquid soap preparations, or be powdered with talc to neutralize the acid or remove unreacted acid. TCA or BCA treatment can be repeated weekly if necessary.Note: TCA solution has a low viscosity comparable with that of water and can spread rapidly and damage adjacent tissues if applied excessively.*Persons with external anal or perianal warts might also have intra-anal warts. Thus, persons with external anal warts might benefit from an inspection of the anal canal by digital examination, standard anoscopy, or high-resolution anoscopy.Source: Workowski KA, Bachmann LH, Chan PA, et al. Sexually transmitted infections treatment guidelines, 2021. Human papillomavirus (HPV) infection: anogenital warts. MMWR Recomm Rep. 2021;70(No. RR-4):1-187. [2021 STI Treatment Guidelines]Table 5. 2021 STI Treatment Guidelines: Anogenital WartsTreatment of Internal Anogenital WartsInternal anogenital warts include urethral meatus, vaginal, cervical, or intra-anal warts. Management of cervical warts or intra-anal warts should include consultation with a specialist.Recommended for Urethral Meatus WartsCryotherapy with liquid nitrogenCryotherapy with liquid nitrogen
Tradename:Health care providers must be trained on the proper use of cryotherapy because over- and under-treatment can result in complications or low efficacy.Recommended for Urethral Meatus WartsSurgical removalSurgical removal
Tradename:Recommended for Vaginal WartsCryotherapy with liquid nitrogenCryotherapy with liquid nitrogen
Tradename:Note: The use of a cryoprobe in the vagina is NOT recommended because of the risk for vaginal perforation and fistula formation.Recommended for Vaginal WartsSurgical removalSurgical removal
Tradename:Recommended for Vaginal WartsTrichloroacetic acid (TCA) or Bichloroacetic acid (BCA) 80-90% solutionA small amount should be applied only to the wartsTrichloroacetic acid (TCA) or Bichloroacetic acid (BCA) 80-90% solution
Tradename:Recommended for Cervical WartsCryotherapy with liquid nitrogenCryotherapy with liquid nitrogen
Tradename:Management of cervical warts should include consultation with a specialist. For women who have exophytic cervical warts, a biopsy evaluation to exclude high-grade SIL must be performed before treatment is initiated.Recommended for Cervical WartsSurgical removalSurgical removal
Tradename:Management of cervical warts should include consultation with a specialist. For women who have exophytic cervical warts, a biopsy evaluation to exclude high-grade SIL must be performed before treatment is initiated.Recommended for Cervical WartsTrichloroacetic acid (TCA) or Bichloroacetic acid (BCA) 80-90% solutionA small amount should be applied only to the warts.Trichloroacetic acid (TCA) or Bichloroacetic acid (BCA) 80-90% solution
Tradename:Management of cervical warts should include consultation with a specialist. For women who have exophytic cervical warts, a biopsy evaluation to exclude high-grade SIL must be performed before treatment is initiated.Recommended for Intra-anal WartsCryotherapy with liquid nitrogenCryotherapy with liquid nitrogen
Tradename:Management of intra-anal warts should include consultation with a specialist. Health care providers must be trained on the proper use of cryotherapy because over- and under-treatment can result in complications or low efficacy.Recommended for Intra-anal WartsSurgical removalSurgical removal
Tradename:Management of intra-anal warts should include consultation with a specialist.Recommended for Intra-anal WartsTrichloroacetic acid (TCA) or Bichloroacetic acid (BCA) 80-90% solutionA small amount should be applied only to the warts.Trichloroacetic acid (TCA) or Bichloroacetic acid (BCA) 80-90% solution
Tradename:Management of intra-anal warts should include consultation with a specialist.Source: Workowski KA, Bachmann LH, Chan PA, et al. Sexually transmitted infections treatment guidelines, 2021. Human papillomavirus (HPV) infection: anogenital warts. MMWR Recomm Rep. 2021;70(No. RR-4):1-187. [2021 STI Treatment Guidelines]Funded byCenters for Disease Control and Prevention
Cooperative Agreement (CDC-RFA-PS20-2004)Created at Part of
Part of CME provided by
CME provided by CNE approved by
CNE approved by
Since you've received 80% or better on this quiz, you may claim continuing education credit.
You seem to have a popup blocker enabled. If you want to skip this dialog please Always allow popup windows for the online course.
Current Version: nstdc-monorepo-0406a550-2025-04-04-232359 - Lesson 2






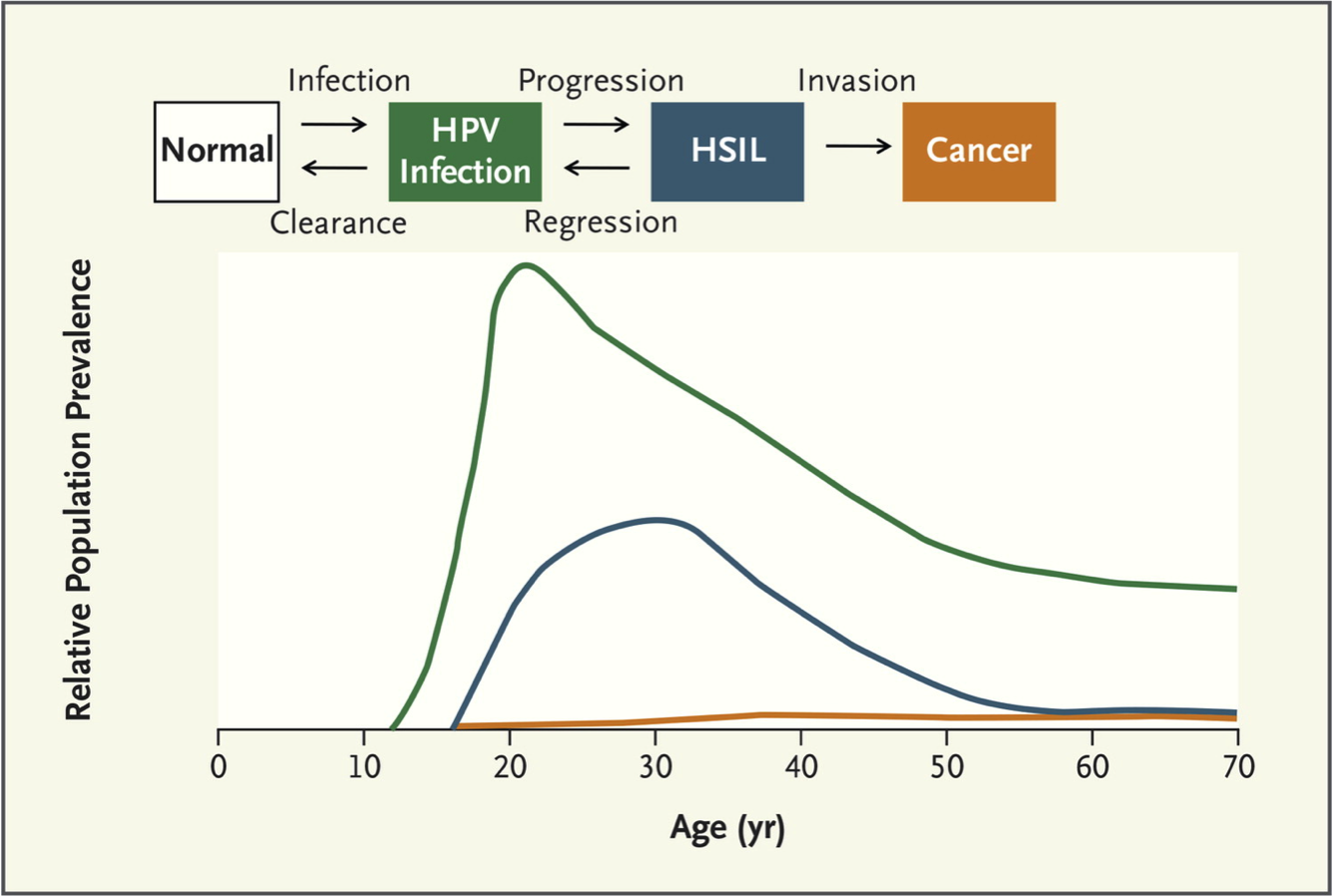







{kind=link}